Infraorbital Nerve Hypoesthesia Secondary to a Benign Maxillary Retention Cyst: Case Report
The retention cyst is a frequent finding in craniofacial massif’s images. They are usually asymptomatic and benign, and do not require endoscopic sinus surgery. There is scarse literature about its implantation on the orbital wall of the maxillary sinus. We present the case of a patient with a maxillary sinus roof cyst, and hypoesthesia in the territory of the infraorbital nerve.
Introduction
Mucous retention cysts of the maxillary sinus are benign and usually asymptomatic lesions, present in up to 14% of adult patients. They generally appear as rounded, dome-shaped soft tissue masses, most often in the floor of the maxillary sinus. They are usually found incidentally on images of the craniofacial area.
The literature reported on maxillary cysts associated with infraorbital involvement is scarce. In this paper we report a case of a periorbital hypesthesia secondary to compression of the infraorbital nerve by a mucous cyst implanted in the roof of the maxillary sinus [1].
Case Report
This is the case of a 37-year-old female patient with a history of rheumatoid arthritis and recurrent herpetic infections, receiving chronic treatment with corticosteroids. He was remitted to the institution due to hypoesthesia in the periorbital region with right auricular irradiation of one year of evolution.
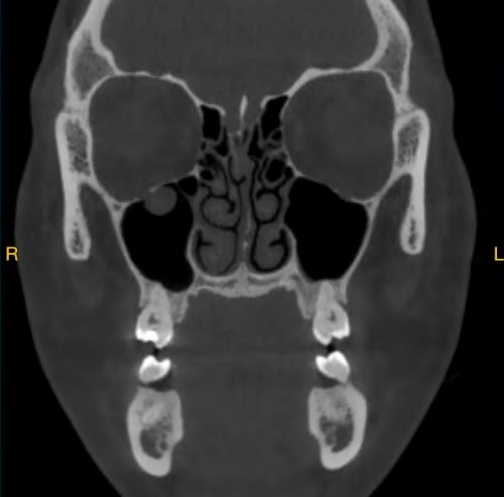
Magnetic resonance imaging of the craniofacial and brain was performed, in which a mass was visualized at the right internal auditory canal compatible with a Schwannoma of the VIII pair. When scrolling the coronal slices of the MRI and computed tomography requested later, a rounded image with homogeneous consistency, regular edges with soft tissue density in computed tomography and hyperintense in T2 in magnetic resonance, was observed. This formation was implanted in the upper wall of the maxillary sinus contacting with the infraorbital nerve (Figures 1-3).


Due to the location and the symptoms reported by the patient, sinonasal endoscopic surgery was performed through an inferior meatotomy approach. The maxillary sinus roof was reached and the pathology was completely excised. Delayed histopathological findings confirmed the diagnosis of mucous retention cyst. Immediately after the intervention, the patient remitted the symptoms.
Discussion
The mucous retention cyst of the maxillary sinus is the most frequent benign solitary lesion of the maxillary sinus. In their pathogenesis, they are formed by the obstruction of a duct of a seromucinous gland of the sinus mucosa, which results in a cystic dilatation of the gland by accumulated mucus. Bradford et al. proposed invagination of the mucosa into the underlying connective tissue as an alternative mechanism for cyst formation. The retention cyst needs to be distinguished from the mucocele, which represents an accumulation of secretion due to a blocked sinus ostium and results in a slow and progressive expansion of the sinus. Other differential diagnoses include pseudocysts, polyps, and tumors, such as lipoma or schwannoma [2].
Retention cysts are believed to be a self-limited condition, with a rate of spontaneous regression and disappearance of 17.6% to 38%.
They are usually asymptomatic. Very infrequently, the sensation of maxillary occupation or pain is described in the literature. The diagnosis is easily made with radiography or computed tomography, where the absence of bone erosion supports the diagnosis. Zago recommends performing an MRI to rule out other possible diagnoses.
For Bradford et al., if the diagnosis is uncertain or the patient atypically presents symptoms, exploration and even biopsy or removal is indicated.
There is few literature reported on retention cysts located at the level of the roof of the maxillary sinus. In this location, compression of the infraorbital nerve in the infraorbital canal is possible, causing the consequent hypoesthesia of the compromised region. The infraorbital canal is constituted with the infraorbital nerve, a branch of V2 from the pterygopalatine fossa, the infraorbital artery, and the infraorbital vein. This nerve is located in the orbital wall of the maxilla and is responsible for the sensory innervation of the skin of the malar area between the lower eyelid and the upper lip [3].
In our case, the removal of the cyst with endoscopic nasal surgery through an inferior meatotomy resulted in the cessation of the patient’s symptoms.
Conclusion
The mucous cyst of the maxillary sinus is a benign lesion and is frequently a radiological finding. Despite its low frequency, the presence of sensitivity disorders in the vicinity of the infraorbital nerve territory should lead to suspicion of compressive nerve injuries and, in such a case, to request images of the craniofacial massif. Lipoma and schwannoma are among the differential diagnoses of the maxillary sinus roof cyst, easily distinguishable by magnetic resonance imaging.
References
-
Sharma N, De M, Pracy P (2007) Recurrent facial paraesthesia secondary to maxillary antral cyst and dehiscent infraorbital canal: case report. J Laryngol Otol 121(6): e6.
-
Zago TM (2018) Infraorbital Neuralgia Secundary to a Retention Mucous Cyst in Maxillary Sinus: A Case Report. Glob J Oto 13(4): 555867.
-
Valverde AL, Diego RGD, Montero J, Albaladejo A (2010) Neuropathic pain associated with mucocele in the maxillary sinus. J Clin Exp Dent 2(3): e142-145.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?