Otosclerosis in Patient with Wilson's Disease
Wilson’s Disease (WD) is a rare genetic disorder characterized by excessive amount of copper stored in body tissues, especially the liver, brain, and corneas of the eyes. Present case study showed otosclerosis in a patient with Wilson’s Disease. Current case study highlights the importance of audiological and otological evaluation in such patients.
Introduction
Copper is a necessary metal in transfer of electron reactions and is desegregated in many cuproenzymes responsible in mitochondrial respiration, antioxidant defense, formation of connective tissues, biosynthesis of neurotransmitter and peptide amidation. However, surplus amount of copper are toxic because they assist the production of reactive oxygen species [1]. One of the disorder of copper metabolism with a identified molecular defect is Wilson’s Disease(WD) [2]. WD is a rare genetic disorder which involves either malabsorption of copper by the body or reduced synthesis of ceruloplasmin [3]. The most common characteristic feature is of WD is the presence of Kayser-Fleischner ring surrounding the cornea [4]. Earlier literature has reported systemic and motor signs with MRI changes within the brainstem and brain [5]. Thomas, et al. [6] reported WD occurs due to ATP7B mutation in the chromosome 13q14.3 and it is a autosomal recessive disease. Early identification and treatment of symptom free WD may be more preferable than the patients with WD having moderate to severe neurological symptoms and liver failure. Neurological symptoms are mainly due to copper toxicity and distinct neuropathological abnormalities [7]. Early neurologic symptoms may be lack of attention and concentration, poor coordination and slurred speech with drooling [8].
Previous investigation has reported hepatic failure, neurological symptoms, psychiatric manifestations, speech disorders, Kayser-Fleisher rings, abnormal fluid retention and jaundice in patients with WD [9, 10, 11]. There is a dearth of literature which has reported hearing loss in patients with WD. Hardin, Barker, et al. [4] highlighted the importance of audiological evaluation in patients with WD. They have also reported unilateral hearing loss (retrocochlear pathology) in patients with WD. Horvath, et al. [12] reported sensorineural hearing loss in a patient with WD. There is a need to explore hearing issues in patients with WD.
In present case study a 21 years old male diagnosed with WD reported with the complaint of reduced hearing sensitivity in right ear. Written informed consent was taken from the patient. Patient’s investigation revealed deranged liver function tests, gait defect, slurred speech and presence of Kayser-Fleisher rings in the patient. CT scan showed atrophic changes in basal ganglia and cerebellar regions. MRI images showed increased signal intensity in the globus pallidus and putamen. Pure tone audiometry and impedance audiometry (tympanometry and reflexometry) were carried out at audiology clinic to diagnose type and degree of hearing loss. Pure tone audiometry was done using modified version of Hughson and Westlake procedure at 250Hz, 500Hz, 1000Hz, 2000Hz, 4000Hz and 8000 Hz for air conduction and 250Hz, 500Hz, 1000Hz, 2000Hz, 4000Hz for bone conduction [13]. Impedance audiometry was investigated (InteracousticAT235, Interacoustic, Denmark) to carry out tympanometry with a probe tone of 226 Hz and ipsilateral and contralateral acoustic reflexes thresholds were obtained at 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz.
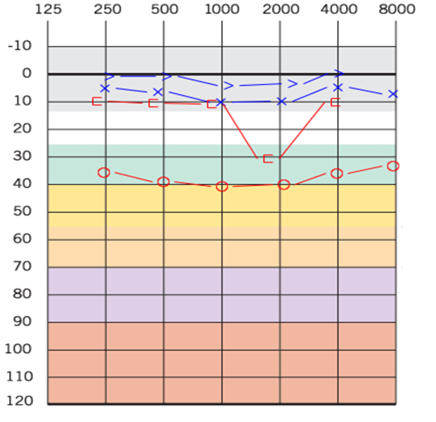
Findings of pure tone audiometry showed mild conductive hearing loss in right ear and normal hearing sensitivity in left ear (Figure 1). Tympanometry revealed As type of tympanogram in right ear and A type in left ear where reflexometry revealed absence of acoustic reflex in right ear whereas acoustic reflex was present in left ear. Right ear audiogram showed a 2KHz BC notch which is the characteristic feature of otosclerosis. Rinne test revealed negative rinne in right ear. Audiological findings revealed otosclerosis in right ear. Explorative tympanotomy was not performed as patient was not willing to undergo any surgical procedure. Patient was not willing to undergo any treatment for hearing loss in right ear.
Discussion
There are no researches, to the best of our knowledge, that have reported otosclerosis in a patient with WD. The outcome of present study revealed otosclerosis in a patient with WD. Previous literature has reported sensorineural hearing loss in a patient with WD [12]. Hardin, et al. [4] also highlighted the importance of audiological evaluations among patients with WD who complains of hearing impairment, tinnitus and intra aural pressure. Surplus of copper in body can lead to hearing loss in patients of WD, possibly by immunological reaction [14, 15]. Immunological abnormalities in patient with WD are caused by liver cirrhosis can be the cause of otosclerosis in our study [15]. Otolaryngologist and audiologist should evaluate and treat hearing loss in these individuals as early as possible.
Conclusions
The present case study highlights the importance of detailed audiological and otological evaluation in patients with WD. Immunological dysfunction in WD can predispose to both sensorineural and conductive hearing loss. Early identification and treatment is essential. More research is needed to point out the exact mechanism and pathophysiology of otosclerosis in WD.
References
-
Kim BE, Nevitt T, Thiele DJ (2008) Mechanisms for copper acquisition, distribution and regulation. Nat Chem Biol 4(3): 176-185.
-
Ferenci P (2004) Pathophysiology and clinical features of Wilson disease. Metab Brain Dis 19(3-4): 229-239.
-
Bandmann O, Weiss KH, Kaler SG (2015) Wilson‘s disease and other neurological copper disorders. Lancet Neurol 14: 103-113.
-
Hardin MF, Barker M, Neis P (2005) Rare auditory- electophysiology finding in Wilson‘s disease. J Ark Med Soc 101: 281-283.
-
Ranjan A, Kalita J, Kumar S, Bhoi SK, Misra UK (2015) A study of MRI changes in Wilson disease and its correlation with clinical features and outcome. Clin Neurol Neurosurg 138: 31-36.
-
Thomas GR, Jensson O, Gudmundsson G, Thorsteinsson L, Cox DW (1995) Wilson disease in Iceland: a clinical and genetic study. Am J Hum Genet 56(5): 1140-1146.
-
Choi BS, Zheng W (2009) Copper transport to the brain by the blood-brain barrier and blood-CSF barrier. Brain Res 1248: 14-21.
-
Machado A, Chien HF, Deguti MM (2006) Neurological manifestations in Wilson‘s disease: Report of 119 cases. Mov Disord 21(12): 2192-1296.
-
Brewer GJ (2001) Zinc acetate for the treatment of Wilson‘s disease. Expert Opin Pharmacother 2(9): 1473- 1477.
-
Merle U, Schaefer M, Ferenci P, Stremmel W (2007) Clinical presentation, diagnosis and long-term outcome of Wilson‘s disease: a cohort study. Gut 56(1): 115-120.
-
Roberts EA, Schilsky ML (2008) Diagnosis and treatment of Wilson disease: an update. Hepatology 47(6): 2089- 2111.
-
Horváth R, Freisinger P, Rubio R (2005) Congenital cataract, muscular hypotonia, developmental delay and sensorineural hearing loss associated with a defect in copper metabolism. J Inherit Metab Dis 28(4): 479-492.
-
Carhart R, Jerger JF (1959) Preferred method for clinical determination of pure-tone thresholds. Journ Sp Lang Hg Diso 24: 330-345.
-
Krysiak R, Handzlik-Orlik G, Okopien B (2012) The role of adipokines in connective tissue diseases. Europ Journ Nut 51: 513-528.
-
Kapoor N, Shetty S, Thomas N, Paul TV (2014) Wilson‘s disease: An endocrine revelation. Indian J Endocrinol Metab 18: 855-857.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?