Cochlear Contrecoup Fracture: A Rare Cause of Sudden Hearing Loss
The temporal bone is the thickest bone in the body and requires a high energy impact to fracture. It contains important structures which can be damaged during impact and cause different types of important complications such as sensorineural hearing loss, facial palsy and vertigo. Sensorineural hearing loss is one of the most relevant lesions when a head trauma occurs. This usually occurs on the ipsilateral side of the lesion. Rarely, it can occur on the contralateral side. A contrecoup injury is defined as an injury that occurs opposite from the side of the blunt. It can happen because of a phenomenon called labyrinthine concussion, described as sensorineural hearing loss with or without labyrinthine symptoms following a head injury without involvement of the otic capsule. We report a case of an uncommon presentation of profound hearing loss due to contrecoup injury with bilateral fracture. In this case, the cochlear implant is considered as an option to improve the patient's quality of life.
Introduction
The temporal bone is the thickest bone in the body and requires a lot of force to fracture, approximately 850 kg lateral force (or 6000 - 8000 N). Injuries to the temporal bone can damage internal structures such as the internal carotid artery, internal jugular vein, VII-XI cranial nerves, and structures in the middle and inner ear. In addition, it can generate damage to the middle cranial fossa, which implies a risk of morbidity and mortality in the patient [1, 2].
Temporal bone fractures occur in 1% to 9% of skull fractures and 36% of basilar skull fractures. The petrous and mastoid portions are the most commonly affected. Physical examination may present with hemotympanum, sensorineural hearing loss, facial palsy and vertigo. Other presentations may include external auditory canal lacerations, tympanic perforations, or mastoid and periorbital ecchymosis [3, 4].
On tomography, fractures can be classified as transverse, longitudinal, or mixed. They can also be classified as fractures with or without involvement of the otic capsule. The most frequent fracture lines are longitudinal and fractures without compromise of the otic capsule. The fracture line provides information about the prognosis and possible complications, such as facial paralysis or hearing loss [5].
Sensorineural hearing loss is one of the serious injuries secondary to trauma, which is usually late diagnosed. This usually occurs on the ipsilateral side of the lesion. Rarely, it can occur on the contralateral side.
One of the theories proposed to explain this phenomenon is the labyrinthine concussion. This phenomenon is described as sensorineural hearing loss with or without labyrinthine symptoms following a head injury without involvement of the otic capsule. A severe blow can generate significant pressure that can be conducted through the bones and injure the organ of Corti, causing reversible or irreversible cell damage. In most cases it involves hearing loss with a scotoma at 4-6 kHz (resembling acoustic trauma, vertigo or tinnitus). In contrast, our case presents as profound hearing loss. Other possible mechanism is labyrinthine hemorrhage or direct damage from a traumatic wave of labyrinthine fluid [6, 7, 8].
Cases of hearing loss contralateral to the injury have been reported in the literature, but in the absence of a fracture line. We report a case of profound hearing loss due to contrecoup with bilateral fracture. A contrecoup injury is defined as an injury that occurs opposite from the point of impact.
Case Report
This is a case of a 57-year-old male patient from Buenos Aires, Argentina who presented at the ENT service of the Higher Otolaryngology Institute with a two-month history of right hearing loss secondary to a 2-meter fall with left side temporoparietal impact. The patient had no associated symptoms. There is no evidence of bruising or injury to the external auditory canal on physical examination. Otomicroscopy confirmed that both ears were ventilated. On acumetric examination, Weber lateralized to the left ear. Rinne had a false negative result in the right ear and positive in the left ear. Vestibular examination was normal and there were no signs of facial nerve palsy.
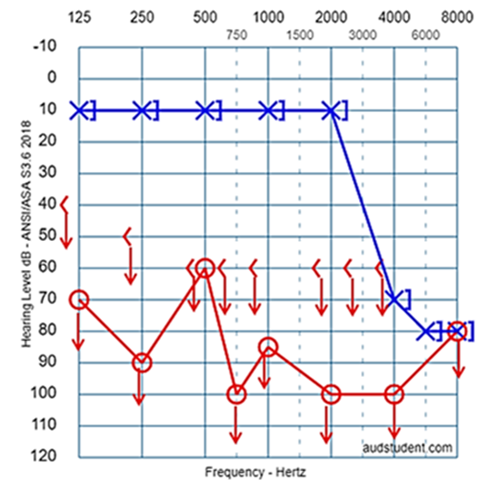
Audiometric studies and cone beam tomography were requested. Pure tone audiometry as shown in Figure 1, revealed profound hearing loss in the right ear and severe hearing loss in 4/6/8 khz without recovery in the left ear. Speech audiometry showed a right ear without discrimination.
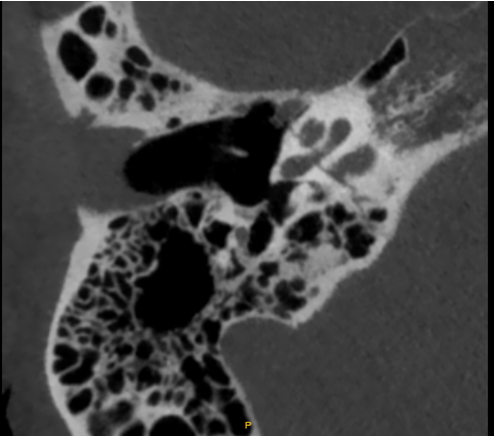
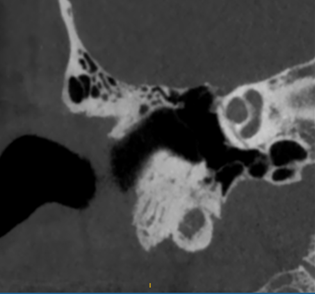
Computed tomography showed a transverse fracture line in the right petrous bone with compromise of the cochlea and the internal auditory canal; and a fracture in the left temporal bone with extension to the mastoid cells, and bilateral superior semicircular canal dehiscence (Figures 2 & 3).
The patient was referred to the Cochlear Implant Center of the Higher Otolaryngology Institute who evaluated the case and proposed a cochlear implant as a good option to improve the patient’s quality of life.
Discussion
The case exposed is a very rare cause of sudden hearing loss. This makes it unique because the impact received on one side of the head generated such a counterforce that fractured the cochlea on the opposite side. Toh [9] presents a case of profound hearing loss in the right ear in a 31-year- old man after a blunt left sided head injury, associated with dizziness and vertigo. No signs of radiologic injury or fistula were found. Two months later, the patient persisted with dizziness and hearing loss.
Temporal bone fractures due to head trauma are not unusual, they can cause complications or sequelae such as facial palsy, conductive or sensorineural hearing loss, cerebrospinal fluid leak, vertigo and vascular lesions. Transverse fractures represent approximately 20% of temporal bone fractures. This type of fracture manifests with severe vestibular or cochlear dysfunction depending on the fracture line. Typical transverse fractures occur in the middle of the skull base on a line that crosses between the middle cranial fossa and the pituitary fossa [10, 11, 12, 13].
When a fracture line involves the cochlea, hearing loss is usually immediate and profound. Lyos11, in a series of three cases, presented a patient with progressive hearing loss secondary to endolymphatic hydrops due to kinetics of the blow.
Most transverse fractures pass through the vestibular aqueduct, generating a series of anatomical changes such as tissue damage, obstruction or fissures. These events are suggested as a potential factor in the genesis of endolymphatic hydrops and therefore the explanation of fluctuating and progressive hearing loss in temporal bone trauma [12].
Ulku, et al. [14] in his study of five transverse fractures of the temporal bone, reported one case of ipsilateral profound hearing loss. The rest of the cases presented House - Brackmann V grade facial palsy. All cases were managed by translabyrinthine decompression. They had functional class improvement to grades II/III.
In a case report published by Zender, et al. [15], he claims to have studied the temporal bones of a patient who died of unknown cause one year after an accident with a fractured temporal bone. It revealed severe microfractures in the cochlea, fissures in the utricle and absence of osteogenesis in the fracture line. This case was also reported with profound hearing loss at the time of the accident.
Ulug, et al. [16] exposes three cases of labyrinthine concussion in contralateral ears in patients who suffered unilateral traumatic fractures of the temporal bone associated with facial palsy. It is similar to our case due to the contralateral hearing condition, however, they differ since these patients had involvement of the seventh cranial nerve and absence of cochlear fracture.
The case we report appears to be the only described in the current available literature. The patient was referred to the Prof. Diamante Cochlear Implant Center as he was a suitable case for a cochlear implant.
Conclusion
This case depicts an uncommon presentation of contralateral profound hearing loss due to a contrecoup transverse temporal bone fracture involving the cochlea. An assessment with magnetic resonance imaging and high- resolution slice tomography is suggested in these patients to determine the integrity of the cochlea and its nerve. Prompt evaluation for cochlear implant candidacy is required in order to avoid the labyrinth ossification.
Topographical and functional detection of the fracture injury will reduce the risk of long-term complications which can occur due to the dynamics of the coup-contrecoup injury.
References
-
Travis LW, Stalnaker RL, Melvin JW (1977) Impact trauma of the human temporal bone. J Trauma 17(10): 761-766.
-
Padmakumar V, Ramesh Kumar E, Ramakrishnan VR (2019) A Prospective Study on Temporal Bone Involvement in Polytrauma Patients and the Effect of Early Diagnosis on Hearing Loss. Indian Journal of Otolaryngology and Head & Neck Surgery 72(1): 30-35.
-
Ricciardiello F, Mazzone S, Longo G, Russo G, Piccirillo E, et al. (2021) Our Experience on Temporal Bone Fractures: Retrospective Analysis of 141 Cases. Journal of Clinical Medicine 10(2): 201.
-
Nicolau LM, Guerra Bru MF, Dellagiovanna M (2021) Fractura de hueso temporal bilateral: reporte de caso. Federación Argentina de Sociedades de Otorrinolaringología 28 (2): 43-47.
-
Carranza RG, Castellano MJ, Chaile ID, Pugliese PM, Romani C, et al. (2015) Anatomía aplicada a fracturas de temporal análisis de 10 casos. Federación Argentina de Sociedades de Otorrinolaringología 22(1): 29-34.
-
Villarreal IM, Méndez D, Silva JMD, Álamo PO del (2016) Contralateral Cochlear Labyrinthine Concussion without Temporal Bone Fracture: Unusual Posttraumatic Consequence. Case Reports in Otolaryngology 2016: 2123182.
-
Khairi M, Irfan M, Rosdan S (2009) Traumatic head injury with contralateral sensorineural hearing loss. Ann Acad Med Singap 38(11): 1017-1018.
-
Bartholomew RA, Lubner RJ, Knoll RM, Ghanad I, Jung D, et al. (2020) Labyrinthine concussion: Historic otopathologic antecedents of a challenging diagnosis. Laryngoscope Investig Otolaryngol 5(2): 267-277.
-
Toh A, Ho EC, Turner N (2010) Contralateral deafness post head injury without temporal bone fractures. American Journal of Otolaryngology 31(1): 54-56.
-
Zhang YL, Wang DS, Yang XA, Yang TF, Zhang F, et al. (2022) Mechanism of transverse fracture of the skull base caused by blunt force to the mandible. Leg Med (Tokyo) 54: 101996.
-
Lyos AT, Marsh MA, Jenkins HA, Coker NJ (1995) Progressive Hearing Loss After Transverse Temporal Bone Fracture. Archives of Otolaryngology-Head and Neck Surgery 121(7): 795-799.
-
Rizvi SS, Gibbin KP (1979) Effect of Transverse Temporal Bone Fracture on the Fluid Compartment of the Inner Ear. Ann Otol Rhinol Laryngol 88(6): 741-748.
-
Lin TF, Huang YC, Wang PC (2002) Isolated Transverse Transcochlear Temporal Bone Fracture. Otology & Neurotology 23(4): 615-616.
-
Ulkü CH, Uyar Y, Kurnaz G (2009) Temporal bone transverse fracture and peripheric facial paralysis: our surgical approach and results. Kulak Burun Bogaz Ihtis Derg 19(5): 259-262.
-
Zehnder A, Merchant SN (2004) Transverse Fracture of the Temporal Bone. Otology & Neurotology 25(5): 852-
-
Ulug T, Ulubil SA (2006) Contralateral labyrinthine concussion in temporal bone fractures. J Otolaryngol 35(6): 380-383.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?