Tranexamic Acid and Application in Otorhinolaryngology: Literature Review
Tranexamic acid (TA) is an antifibrinolytic drug used for the control of hemorrhages in the different disciplines of medicine. In otorhinolaryngology (ENT) it has multiple applications, both surgical and non-surgical, however, its effectiveness and safety have been controversial over time. Below is a review of the literature regarding this drug and its use in ENT, for divulgation in our environment.
Introduction
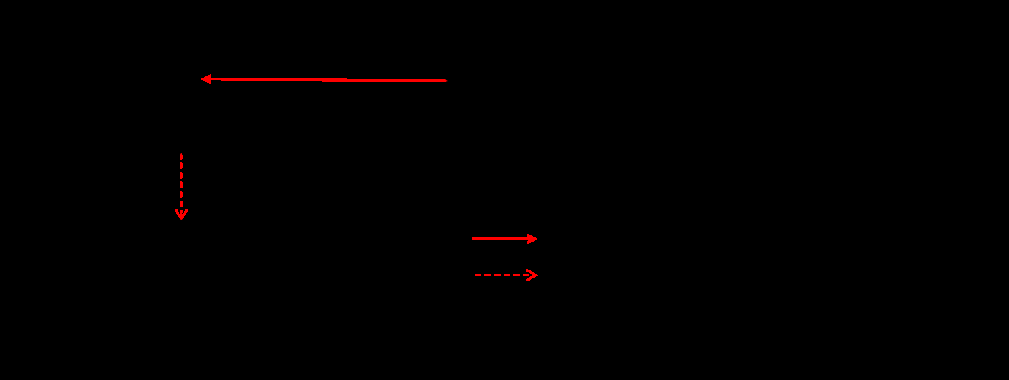
TA is an antifibrinolytic drug whose mechanism of action is to interfere in the coagulation cascade by blocking the formation of plasmin and stabilizing the formed platelet plaques. This is achieved as it is a synthetic analog of the amino acid lysine that binds and competitively blocks plasminogen molecules, which finally manages to inhibit the degradation of already formed plaques [1, 2, 3]. It is also thought to have an anti-inflammatory effect by inhibiting the activation of neutrophils, monocytes and complement by plasmin (Figure 1) [4].
Although the United States Food and Drug Administration (FDA) has only approved its use for heavy menstrual bleeding and as prevention in procedures for patients with hemophilia [5], its indication has been expanded both in the Emergency Room (ER) in the context of patients with polytraumatisms or upper gastrointestinal bleeding as well as in elective surgeries of different specialties (cardiac, trauma, maxillofacial, and others) [1, 2, 3, 4, 6, 7, 8], which practice has not been exempt from controversies regarding to its safety and efficacy.
TA is actualluy available in tablet presentation with a maximum dose of 1 to 1.5 grams every eight to twelve hours, having a bioavailability of 30-50% with a half-life of 2-3 hours. It can also be indicated intravenously with 0.5 to 1 gram every eight hours. The renal function of the patients must be taken into consideration and the dosage adjusted if is necessary (Table 1) [9], since 95% is excreted through this route [4, 10].
| Condition | Dose | |
|---|---|---|
| Intravenous | Creatinine <1.4mg/dL | No adjustment required: 10 mg/kg or 1 g 3 to 4 times a day |
| Intravenous | Creatinine ≥ 1.4 a <2.8 mg/dL | Usual dose 2 times a day |
| Intravenous | Creatinine ≥ 2.8 a <5.7 mg/dL | Usual dose 1 time a day |
| Intravenous | Creatinine ≥ 5.7 mg/dL Triweekly hemodialysis Peritoneum dialysis | Usual dose every 48 hours or 50% of the usual dose every 24 hours |
| Oral | Creatinine <1.4mg/dL | No adjustment required: 10-15 mg/kg or 1-1.5 g 4 times a day |
| Oral | Creatinine ≥ 1.4 a <2.8 mg/dL | Usual dose 2 times a day |
| Oral | Creatinine ≥ 2.8 a <5.7 mg/dL | Usual dose 1 time a day |
| Oral | Creatinine ≥ 5.7 mg/dL Triweekly hemodialysis Peritoneum dialysis | Usual dose every 48 hours or 50% of the usual dose every 24 hours |
Table 1: Dose adjustment of tranexamic acid in patients with kidney damage.
There are adverse reactions to the use of AT, which are mostly mild, highlighting the gastrointestinal ones such as nausea and diarrhea, however, there are reports of cases of thromboembolic events and seizures, the latter in the context of high doses and in patients who were undergoing open heart surgery, however it is recommended not to administer it to neurosurgical patients or patients with a history of epilepsy [4]. It is important to consider the contraindications of this drug, being absolute in the case of isolated traumatic brain injury, increased risk of thrombosis, hypersensitivity to TA, active intravascular coagulation and subarachnoid hemorrhage (due to increased risk of cerebral edema); and relative, advising its use with caution, in those patients with thromboembolic disease, those with bleeding from the upper urinary tract or ureteral obstruction due to clots, or its concomitant use with some procoagulant drugs such as factor IX concentrates [11, 12].
Below, we present a summary of the current evidence related to TA and its use in ENT, to facilitate its use in the prevention and treatment of bleeding and its complications.
Uses of TA in ENT
Epistaxis: Epistaxis corresponds to bleeding from the nostrils, it is a common symptom within the general population, with an incidence of at least 60%, of these
10% may require attention in ER. Epistaxis has a bimodal presentation, with a higher incidence in childhood and in older adult patients. 90% of the episodes correspond to anterior epistaxis (compromising Kiesselbach’s plexus) and the remaining percentage results from posterior epistaxis (Woodruff’s plexus) [13, 14]. The last American guideline on epistaxis that was published in 2020 indicates a proposal for the management of epistaxis that begins with compressive measures in the case of being active, associated or not with topical vasoconstrictors, nasal cauterization if the site of bleeding can be identified and if it is not possible observe it, anterior or posterior nasal packing is recommended if the first is frustrating. Regarding the use of tranexamic acid, it mentions that due to the lack of contemporary studies that evaluate the oral and topical use of TA in the management of epistaxis, new studies are required to include this drug in the treatment of nasal bleeding [14].
In 2018, Joseph, et al. [1] publish a meta-analysis that includes six randomized controlled trials (RCT) whose main objective was to determine the effects of TA in any of its presentations compared to placebo or other hemostatic agents in patient’s whit epistaxis. Six RCT with a total of 692 participants were included. In the two studies that compared oral TA (administered for one week) versus placebo, a reduction in the risk of re-bleeding in the following 10 days was shown from 69% to 49% with a relative risk (RR) of
0.73. The time to cessation of bleeding in these cases was not reported. Another study compared the topical use of TA versus placebo, a reduction from 66% to 43% was observed, with a RR of 0.66, however the study was considered as low-quality evidence. The remaining analyzes compared TA with other hemostatic agents such as phenylephrine plus lidocaine, it was determined that the time to cessation of epistaxis was significantly shorter in the AT group (70% versus 30% with RR 2.35).
Robb, et al. [15] conducted a review of the literature on the use of TA in ENT, regarding the management of epistaxis, a RCT that compared the effect on the reduction of bleeding time by administering a single intravenous injection of 500 mg of AT with the use of anterior packing (using a tetracycline and vasoconstrictor solution), showing a faster stoppage of nasal bleeding at 10 minutes by the group with AT, in addition to a decrease in rebleeding at 24 hours and improvement in patient satisfaction, which is why the authors recommend TA as the initial treatment of anterior epistaxis.
However, given the fact that there have only been 3 RCTs about uses of TA in patients with epistaxis between 1995 and 2018, new studies incorporating AT in the management of epistaxis, and considering different routes of administration and doses, in different age groups, where the complications resulting from the use of the same drug are considered, could be relevant to evaluate the effectiveness of TA in the control of epistaxis [1, 15].
It is important to mention groups of patients with special characteristics such as those who use antiplatelet treatment with aspirin or clopidogrel. There is a prospective, double- blind, randomized study that compares the use of topical TA versus the use of anterior tamponade with phenylephrine in these patients. 100 patients were studied and it was concluded that with the use of TA there was a decrease in bleeding time and less recurrence, so the use of topical AT was recommended in this group of patients [16].
Another particular group of patients are those with epistaxis related to Rendu-Osler-Weber Syndrome or hereditary hemorrhagic telangiectasia (HHT), which is its main symptom, with evidence supporting the use of TA to control epistaxis by reducing the duration of epistaxis itself and the number of monthly episodes of nasal bleeding, with contradictory information regarding the usefulness of its topical administration [17, 18].
ENT Surgery
Minor oral surgery: The topical use of TA has been studied in patients using oral anticoagulants in minor surgical procedures of the oral cavity. De Vasconcelos, et al. [19] carried out a meta-analysis in which they evaluate the use of TA in dental procedures, including dental and third molar extractions, showing its effectiveness and safety in reducing postoperative bleeding when daily mouthwashes are performed during the first postoperative week. In the same study, as a secondary result, no case of thromboembolic events during the first postoperative week was reported. On the other hand, in minor oral ENT surgery itself, studies are needed to evaluate the use of TA for the control of perioperative bleeding. It is thought that the effect of TA in these surgeries is due to the inhibition of fibrinolytic enzymes present in saliva [4].
Head and Neck Surgeries
In recent years, randomized studies have been carried out to achieve the use of TA in this type of surgery. Chen, et al. [20] evaluated the use of TA during anesthetic induction (in dose of 10mg/kg IV) and intraoperatively (1mg/kg/h IV) in patients undergoing modified radical cervical dissections, suprafacial hemithyroidectomies and parotidectomies, observing a significant decrease in postoperative bleeding in comparison with the control group. Subsequently, other authors have evaluated its use in unilateral oncological surgery of the oral cavity, supraomohyoid neck dissections, modified radical neck dissections, mandibular resection and flap reconstructions, concluding that using TA during anesthetic induction (10-20mg/kg IV) reduced the intraoperative blood loss [21, 22]. Recently, the meta-analysis carried out by Alsubai, et al. [23] reports that the use of TA significantly reduces the volume of intraoperative bleeding; however, it does not improve post-surgery hemoglobin levels, neither the days with drainage or the time of surgery.
Tonsilectomy
Tonsillectomy is one of the most common surgical procedures in ENT. Among its most severe complications are post-surgical hemorrhage and death11. Regarding postsurgical hemorrhage, it is divided into primary (within the first 24 hours) and secondary (after the first 24 hours) [2].
A significant number of papers have been published with variable results for post-tonsillectomy bleeding using different antifibrinolytic agents. In a review of the literature and meta-analysis, it was shown that the use of intravenous TA during surgery reduced the volume of bleeding, however it was not possible to demonstrate a reduction in the rate of post-surgical bleeding, this was explained by the short half- life of TA that it would have no effect on secondary bleeding if it was given in a single dose on the day of surgery [15].
Koizumi, et al. [2] report contrary results when studying a cohort of nearly 110,000 patients from 745 hospitals who had undergone tonsillectomy. They compared two groups: those who had received TA from day one of the surgical intervention (n=50,501) with those without the use of the drug (n=60,427), concluding that the administration of TA from the very day of the tonsillectomy would not reduce the risk of surgical reintervention due to secondary bleeding or blood transfusion, despite its safety. In addition, it was shown that TA is not effective in reducing post-surgical hemorrhage, this was explained because secondary bleeding (after the first 24 hours) generally occurs when the tonsillar bed scar falls prematurely due to mechanical trauma (from meals, for example) before the surgical site is completely healthy, therefore, AT-mediated fibrin clot stabilization cannot prevent secondary bleeding.
On the other hand, Chan, et al. [11] carried out a systematic review and meta-analysis on the use of TA in tonsillectomy, reporting safety and a significant reduction in the volume and duration of bleeding using topical TA, but not in the number of patients who develops post-tonsillectomy hemorrhage. In other meta-analysis carried out in 2021 reports that the use of TA reduces intraoperative bleeding by 39 ml on average and reduces the risk of post-tonsillectomy bleeding by 58% [24].
Schwarz, et al. [3] reported a case of a 3-year-old patient, who on his fourth day after tonsillectomy and adenoidectomy presented in the ER with post-surgical hemorrhage, recommending, in the first instance, management with epinephrine nebulization and, if required, proceed with nebulized AT at a dose of 10 mg/kg (ampoules of 100 mg/L), at a flow of 8 L/min for 2 to 3 minutes, although in general terms doses of 250 mg are considered for children weighing less than 25 kg , while for weights greater than 25 kg the dose amounts to 500 mg; all this, while airway management is being prepared and the surgical teams are being activated. For the adult population, the dose of nebulized AT corresponds to 1 gr. Although no adverse effects have been observed in the pediatric population after administration by nebulization of TA due to epistaxis, there is a report of 1 case in the adult population that presented bronchospasm, which in turn was reversed with the use of bronchodilators.
In relation to topical use, Falbe-Hansen, et al. [25] carried out a prospective, double-blind study in which he evaluated the use of TA gel that was applied in the tonsillar fossa in gauzes 4 minutes after tonsillectomy, its results showed that there was no decrease in the risk of subsequent bleeding, nor in a lower decrease in hemoglobin and hematocrit in these patients when using topical TA versus placebo. Hinder, et al. [26] similarly, when using TA solution gargles, concluded that its use does not reduce the risk of postoperative bleeding or the risk of surgical intervention secondary to it.
Although there are multiple studies regarding the use of TA in tonsillectomy, at the time of performing meta-analyses very few manage to be included, concluding its safety of use and the reduction of intraoperative bleeding, but not its effectiveness in reducing post-tonsillectomy hemorrhage [15]. Most authors mention the lack of evidence in this topic and the need for future studies [11, 15].
Adenoidectomy
There is a lack of studies regarding the use of TA in this surgical procedure [15]. The effects of TA in this surgery are extrapolated from patients who have undergone adenotonsillectomy, showing that the use of TA does not significantly reduce bleeding in patients undergoing adenoidectomy or tonsillectomy. However, in those who go to adenotonsillectomy, a significant reduction is observed with its use [27].
Albirmawy, et al. [28] showed a decrease in the volume of intraoperative blood loss and a decrease in primary postoperative bleeding (first 24 hours) with the topical use of 1 g of TA in 10 ml of 0.9% saline solution irrigated through a catheter in the nasopharynx for 5 minutes post adenoidectomy, compared with placebo, in a group of 400 children.
Rhinoplasty
A successful rhinoplasty requires a detailed understanding of the nasal structure necessary to produce a functional and aesthetically pleasing nose. In addition to this, a thorough surgical technique and the management of postoperative edema are essential to achieve the results proposed and requested by each patient. Among the complications, bleeding, ecchymosis, and edema are usually the most frequent, and can cause great concern and discomfort in patients, and can lead to the development of infections with the consequent catastrophic result from the aesthetic point of view and even on rare occasions cause death [29, 30, 31]. The use of TA has been postulated as a tool to reduce these complications, during the last years 4 meta- analyses have been published. De Vasconcellos, et al. [32] and McGuire, et al. [33] included in their analysis 5 RCT that showed a decrease in intraoperative bleeding. The schemes used vary among them, however, most include a dose prior to surgery of 10mg/kg IV and some of them indicate 1 g every 8 hours for 1 to 5 days after surgery. Additionally, Ping et al. has reported a significant decrease in eyelid edema and postoperative ecchymosis [34]. The latest meta-analysis published in 2022 by Laikhter, et al. [35] confirms the results obtained previously.
Nasal Endoscopic Surgery (ENS)
ENS requires a visible surgical field for proper recognition of anatomical points in order to avoid complications such as injury to the skull base or orbit, so different techniques have been used to minimize intraoperative bleeding with agents such as epinephrine either topical or injected into the lateral nasal wall, the use of total intravenous anesthesia (TIVA), controlled hypotension and the patient’s position with the head at 30º in relation to the horizontal [36].
Langille, et al. [37] describe a RCT in 28 patients undergoing ENS for chronic rhinosinusitis with or without polyps. The patients were divided into two groups: half were prescribed 1 gram of intravenous TA as premedication and the other half was the control group to which this antifibrinolytic was not indicated. It was concluded in this study that TA did not show a decrease in intraoperative bleeding and improvement in visibility in relation to cases that did not have premedication with TA.
Another study compared 200 patients who underwent nasal endoscopic surgery for different reasons (septoplasty, chronic rhinosinusitis, tumor excision, among others), half of whom were prescribed TA as premedication in infusion (500 mg in 100 mL of solution saline for 20 to 30 minutes) and the other half was the control group. It was observed that in the first group there was a decrease in the volume of blood lost by 72.48%, and no adverse effects were reported. In addition, the authors noted that the antifibrinolytic effect lasted up to 8 hours in plasma, reducing the possibility of postoperative bleeding [38].
A meta-analysis carried out by Kang, et al. [39] in 2019 that included 4 primary studies with a total of 226 patients that compared the topical use of TA during surgery with various controls such as its non-use or the use of saline solution, concluded that its use reduced bleeding intraoperatively, as well as improves the visibility of the surgical field.
Conclusion
Hemorrhage, both primary and secondary to surgical interventions and others, is a common reason for consultation in ENT, both in the pediatric and adult population, in which the use of TA within the therapeutic scheme should be considered, since the existing evidence to date refers to decreased bleeding, evolution time, patient satisfaction and decreased costs associated with morbidity. Despite the above, modern studies focused on specific groups are necessary to be able to establish treatment schemes applicable on a large scale within our environment.
References
-
Joseph J, Martinez-Devesa P, Bellorini J, Burton MJ (2018) Tranexamic acid for patients with nasal haemorrhage (epistaxis). Cochrane Database of Systematic Reviews 12(12).
-
Koizumi M, Ishimaru M, Matsui H, Fushimi K, Yamasoba T, et l. (2019) Tranexamic acid and post-tonsillectomy hemorrhage: propensity score and instrumental variable analyses. European Archives of Oto-Rhino-Laryngology 276(1): 249-254.
-
Schwarz W, Ruttan T, Bundick K (2019) Nebulized Tranexamic Acid Use for Pediatric Secondary Post- Tonsillectomy Hemorrhage. Annals of Emergency Medicine 73(3): 269-271.
-
Reed MR, Woolley LT (2015) Uses of tranexamic acid. Continuing Education in Anaesthesia Critical Care & Pain 15(1): 32-37.
-
Chauncey JM, Wieters JS (2022) Tranexamic Acid. BJA 15(1): 32-37.
-
Perel P, Ker K, Morales Uribe CH, Roberts I (2013) Tranexamic acid for reducing mortality in emergency and urgent surgery. Cochrane Database of Systematic Reviews 2013(3).
-
Ker K, Beecher D, Roberts I (2013) Topical application of tranexamic acid for the reduction of bleeding. In: Ker K, ed. Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd, 2013.
-
Evaniew N, Bhandari M (2017) Cochrane in CORR ®: Topical Application of Tranexamic Acid for the Reduction of Bleeding (Review). Clinical Orthopaedics & Related Research 475(1): 21-26.
-
Andersson L, Eriksson O, Hedlund PO, Kjellman H, Lindqvist B (1978) Special considerations with regard to the dosage of tranexamic acid in patients with chronic renal diseases. Urological Research. 6(2).
-
McCormack PL (2012) Tranexamic Acid. Drugs 72(5): 585-617.
-
Chan CC, Chan YY, Tanweer F (2013) Systematic review and meta-analysis of the use of tranexamic acid in tonsillectomy. European Archives of Oto-Rhino- Laryngology 270(2): 735-748.
-
Gaines-Dillard N, Bartley MK, Rosini JM (2016) Ácido tranexámico en el paciente con traumatismos. Nursing (Ed Española) 33(5): 33-35.
-
Camila L, Diaz B, Vargas A, Ruiz S, Libieth M, et al. (2021) Update on the approach to epistaxis in children and adults. Scientific & Educational Medical Journal 1: 33.
-
Tunkel DE, Anne S, Payne SC (2020) Clinical Practice Guideline: Nosebleed (Epistaxis). Otolaryngology–Head and Neck Surgery 162(S1): S1-S38.
-
Robb PJ (2014) Tranexamic acid-a useful drug in ENT surgery?. The Journal of Laryngology & Otology 128(7): 574-579.
-
Amini K, Arabzadeh A, Jahed S, Amini P (2021) Topical Tranexamic Acid versus Phenylephrine-lidocaine for the Treatment of Anterior Epistaxis in Patients Taking Aspirin or Clopidogrel; a Randomized Clinical Trial. Arch Acad Emerg Med 9(1): e6.
-
Gaillard S, Dupuis-Girod S, Boutitie F (2014) Tranexamic acid for epistaxis in hereditary hemorrhagic telangiectasia patients: a European cross-over controlled trial in a rare disease. Journal of Thrombosis and Haemostasis 12(9): 1494-1502.
-
Whitehead KJ, Sautter NB, McWilliams JP (2016) Effect of Topical Intranasal Therapy on Epistaxis Frequency in Patients with Hereditary Hemorrhagic Telangiectasia. JAMA 316(9): 943.
-
De Vasconcellos SJ de A, De Santana Santos T, Reinheimer DM, Faria-e-Silva AL, De Melo M de FB, et al. (2017) Topical application of tranexamic acid in anticoagulated patients undergoing minor oral surgery: A systematic review and meta-analysis of randomized clinical trials. Journal of Cranio-Maxillofacial Surgery 45(1): 20-26.
-
Chen CC, Wang CC, Wang CP, Lin TH, Lin WD, et al. (2008) Prospective, randomized, controlled trial of tranexamic acid in patients who undergo head and neck procedures. Otolaryngology–Head and Neck Surgery 138(6): 762- 767.
-
Das A, Chattopadhyay S, Mandal D (2015) Does the preoperative administration of tranexamic acid reduce perioperative blood loss and transfusion requirements after head neck cancer surgery? A randomized, controlled trial. Anesthesia: Essays and Researches 9(3): 384.
-
Kulkarni A, Chaukar D, Patil V, Metgudmath R, Hawaldar R, et al. (2016) Does tranexamic acid reduce blood loss during head and neck cancer surgery?. Indian Journal of Anaesthesia 60(1): 19.
-
Alsubaie HM, Abu Zaid A, Sayed SI (2022) Tranexamic acid in head and neck procedures: a systematic review and meta-analysis of randomized controlled trials. European Archives of Oto-Rhino-Laryngology 279(5): 2231-2238.
-
Kuo CC, DeGiovanni JC, Carr MM (2021) The efficacy of Tranexamic Acid Administration in Patients Undergoing Tonsillectomy: An Updated Meta-Analysis. Annals of Otology, Rhinology and Laryngology 131(8): 834-843.
-
Falbe-Hansen J, Jacobsen BO, Lorexzen E (1974) Local Application of an Antifibrinolytic in Tonsillectomy A Double-Blind Study. J Laryngol Otol 88(6): 565-568.
-
Hinder D, Tschopp K (2014) Topische Anwendung von Tranexamsäure zur Prophylaxe von Nachblutungen nach Tonsillektomie. Laryngo-Rhino-Otologie 94(02): 86-90.
-
Verstraete M, Tyberghein J, Greef Y de, Daems L, Hoof A van (1977) Double-Blind Trials with Ethamsylate, Batroxobin or Tranexamic Acid on Blood Loss After Adenotonsillectomy. Acta Clinica Belgica 32(2): 136-141.
-
Albirmawy OA, Saafan ME, Shehata EM, Basuni AS, Eldaba AA (2013) Topical application of tranexamic acid after adenoidectomy: A double-blind, prospective, randomized, controlled study. International Journal of Pediatric Otorhinolaryngology 77(7): 1139-1142.
-
Perrotta PL, Snyder EL (2001) Non-infectious complications of transfusion therapy. Blood Reviews. 15(2): 69-83.
-
Berkowitz RL (2018) Commentary on: “Comparison of the Effect of Dexamethasone and Tranexamic Acid, Separately or in Combination on Post-rhinoplasty and Edema and Ecchymosis.” Aesthetic Plastic Surgery 42(1): 253-255.
-
Totonchi A, Guyuron B (2007) A Randomized, Controlled Comparison between Arnica and Steroids in the Management of Postrhinoplasty Ecchymosis and Edema. Plastic and Reconstructive Surgery 120(1): 271-274.
-
De Vasconcellos SJ de A, do Nascimento-Júnior EM, De Aguiar Menezes MV, Tavares Mendes ML, de Souza Dantas R, et al. (2018) Preoperative Tranexamic Acid for Treatment of Bleeding, Edema, and Ecchymosis in Patients Undergoing Rhinoplasty. JAMA Otolaryngology– Head & Neck Surgery 144(9): 816.
-
McGuire C, Nurmsoo S, Samargandi OA, Bezuhly M (2019) Role of Tranexamic Acid in Reducing Intraoperative Blood Loss and Postoperative Edema and Ecchymosis in Primary Elective Rhinoplasty. JAMA Facial Plastic Surgery 21(3): 191-198.
-
Dong PW, Ming ZQ, Feng SH, Shan LH, Li F (2019) Role of tranexamic acid in nasal surgery review and meta- analysis of randomized control trial. Medicine 98(16): e15202.
-
Laikhter E, Comer CD, Shiah E, Manstein SM, Bain PA, et al. (2022) A Systematic Review and Meta-Analysis Evaluating the Impact of Tranexamic Acid Administration in Aesthetic Plastic Surgery. Aesthetic Surgery Journal 42(5): 548-558.
-
Wormald P (2017) Endoscopic Sinus Surgery: Anatomy, Three-Dimensional Reconstruction, and Surgical Technique. In: 4th (Edn.), pp: 320.
-
Langille MA, Chiarella A, Côté DWJ (2013) Intravenous tranexamic acid and intraoperative visualization during functional endoscopic sinus surgery: a double-blind randomized controlled trial. International Forum of Allergy & Rhinology 3(4): 315-318.
-
Chhapola S, Matta I (2011) Short-term Use of Tranexamic Acid to Reduce Blood Loss in Endoscopic Nasal Surgeries. An International Journal Clinical Rhinology 4(2): 79-81.
-
Kang H, Hwang SH (2020) Does topical application of tranexamic acid reduce intraoperative bleeding in sinus surgery during general anesthesia? Brazilian Journal of Otorhinolaryngology 86(1): 111-118.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?