A Case of Laryngitis without Hoarseness Caused by Coxsackie virus In Group B
A rare laryngitis patient who had no obvious inducement to severe laryngeal pain but had silent hoarseness, laryngoscopy showed only herpes, congestion and edema in the laryngeal cavity mucosa. After intravenous administration of acyclovir and methylprednisolone, the symptoms of laryngeal pain were significantly alleviated on the same day and recovered in 5 days. Through the diagnosis and treatment of this patient, it is suggested that Coxsackie virus B can only invade the laryngeal cavity mucosa and sensory nerve endings without invading the vocal cords.
Introduction
In the outpatient department of laryngology, acute laryngitis is a common disease, often with hoarseness and sore throat as the main complaints [1]. The author received a patient with laryngitis who complained of severe sore throat but had no hoarseness in the throat clinic. The laboratory test showed that Coxsackie virus B IgM antibody was weakly positive, so he was diagnosed as Coxsackie virus laryngitis. Through literature review, there is no relevant report on Coxsackie viral laryngitis [2], which is reported below.
Case Presentation
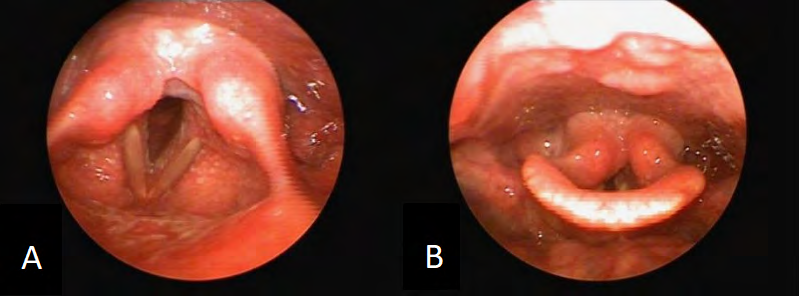
The patient is a 43 year old female. There is no obvious inducement for throat discomfort to worsen for 3 days, and the pain is unbearable for 1 day. The laryngoscopy showed that the laryngeal cavity mucosa showed granular and patchy herpetic lesions, the vocal cord morphology and movement were normal, and no abnormality was found in the throat mucosa. See Figure AB Laboratory examination: Coxsackie virus type B IgM antibody is weakly positive, herpes simplex virus type I, herpes simplex virus type II, varicella zoster virus, respiratory syncytial virus, adenovirus, influenza virus type A, influenza virus type B, parainfluenza virus, chlamydia pneumoniae, Coxsackie virus type A, Ecovirus, Mycoplasma pneumoniae legionella pneumophila IgM is negative, C-reactive protein 12.2mg/L (0-3.0), erythrocyte sedimentation rate 24mm/L (0-20), blood routine is normal, ECG is normal.
Previous history: healthy, denied history of diabetes, hypertension, etc. Treatment: 1. 0.9% sodium chloride 250ml+ribavirin 500mg, qd, ivgtt, 5 days; 2. 0.9% sodium chloride 150ml+methylprednisolone 120mg, qd, ivgtt, 3 days, cured (Figure 1).
Discussion
Acute laryngitis is an acute inflammation of laryngeal mucosa, which occurs frequently in winter and spring. It is a common acute respiratory infectious diseases. The main complaints are hoarseness and sore throat. The causes are mainly influenza virus, parainfluenza virus, rhinovirus, adenovirus, hemolytic streptococcus, pneumococcus and other pathogenic microorganisms, which can be accompanied by chills, fever, and general weakness [1]. This patient only had isolated severe throat pain, without hoarseness, cough, chills, fever, etc. Laryngoscopy showed congestion and patchy herpetic lesions in epiglottic laryngeal surface and laryngeal cavity mucosa, and no abnormality was found in bilateral vocal cords and pharyngeal cavity oral mucosa. Serological examination showed only weak positive Coxsackie virus group B IgM, but no positive herpes simplex virus type I, type II, varicella zoster virus IgM, indicating that the laryngeal cavity mucosa herpes of this patient was caused by infection of Coxsackie virus group B in the acute phase, rather than herpes simplex virus type I, type II, varicella zoster virus infection. Reviewing the literature on acute laryngitis and Coxsackie virus group B disease at home and abroad, most of them are about oral and pharyngeal isthmus, hand and foot herpes, myocarditis, etc. caused by Coxsackie virus group B infection, and no isolated laryngitis caused by laryngeal cavity mucosa or epiglottic and laryngeal lateral herpes is found, so this case is rare [2]. Generally speaking, there is no specific drug for the body damage caused by Coxsackie virus infection. It mainly depends on the self immunity to gradually recover. The course of the disease is generally a few days for mild cases and weeks for severe cases and gradually evolves [3]. However, this patient had severe throat pain at the time of treatment. However, the throat pain was obviously relieved after intravenous administration of acyclovir and methylprednisolone on the same day, and the patient recovered after 5 days of treatment. In a word, this patient has the following rare clinical features:
- Severe throat pain, no hoarseness, and only white granular and patchy herpetic lesions were seen in the laryngeal cavity mucosa under laryngoscope;
- Laboratory serological examination showed that Coxsackie virus group B was weakly positive, indicating that it was caused by Cassackie virus group B infection;
- Acyclovir and methylprednisolone were given intravenously on the same day and recovered on 5 days;
- According to the medical history, there is no person infected with Coxsackie virus in close contact with family members, and the source of infection is not obvious;
- No organ damage such as heart, hand, foot and mouth.
Among them, the rapid effect of acyclovir and methylprednisolone used in 3 cases may be mainly due to the anti-inflammatory effect of methylprednisolone rather than the antiviral effect of acyclovir, because the antiviral mechanism of acyclovir is mainly to inhibit the replication of DNA virus, while coxsackievirus belongs to RNA virus [4]. So why didn’t you use anti RNA drugs such as ribavirin? At the time of receiving the patient, the hospital pharmacy stopped taking ribavirin. Among them, 4 sources of infection are not obvious, which may be caused by recessive infection among close contacts or asymptomatic carriers [5]. Therefore, this patient is an isolated herpetic lesion of the laryngeal cavity mucosa without a clear route of infection and transmission, and it is rapidly effective and cured after intravenous administration of acyclovir and methylprednisolone. So far, there is no relevant report, which has certain clinical reference value.
References
-
Yongquan T (2018) Otolaryngology Head and Neck Surgery. In: 9th (Edn.), People’s Health Publishing House, pp: 328.
-
Conrad Stöppler M (2020) Hoarse Voice and Mouth Sores [J/OL].
-
Xiaoyu Z, Zhiyong W (2010) Manual on Prevention and Treatment of Hand, Foot and Mouth Disease, Gansu Science and Technology Press.
-
Baofeng Y, Jianguo C (2018) Pharmacology. In: 9th (Edn.), People’s Health Publishing House, pp: 409-416.
-
Weimin C (2017) Graphic virus. In: 1st (Edn.), Hubei Science and Technology Press, pp: 58-61.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?