Buccinator Flap in Reconstruction of the Floor of the Mouth: A Case Report
The reconstruction of defects in the oral cavity after oncological resections can be performed with different techniques. Small and moderate defects can be reconstructed with local flaps. The buccinator myomucosal flap has the advantages of being in the same surgical field, have a similar tissue to the area to be reconstructed and due to its different vascular pedicles, it allows various rotation options. We describe the case of a patient who had a squamous cell carcinoma in the floor of the mouth, in whom a resection of the tumor and a marginal mandibulectomy were performed. The defect was successfully reconstructed with a buccinator myomucosal flap with an anterior inferior pedicle.
Introduction
The reconstruction of defects in the floor of the mouth after oncological resections for malignant tumors, can be performed with different techniques. The use of free skin grafts can be useful in small defects in the oral cavity to repair mucosal loss and prevent retraction that can cause secondary scarring. Local flaps can also be used to repair small or medium defects of the floor of the mouth, oral tongue, or palate. The nasogenian flap is a good option to repair the same regions, but it leaves a scar on the face.
The buccinator myomucosal flap (BMF) has the advantage of allowing the reconstruction of different places in the oral cavity due to the different rotation options and does not leave facial scars.
We describe the case of a woman who had a squamous cell carcinoma located in the lateral floor of the mouth with compromise of the mandibular periosteum. Reconstruction of the mucosal and bone defect due to the marginal resection of the mandible was performed with a buccinator myomucosal flap.
Clinical Case
Sixty One Years-Old Woman
She had a history of smoking (15 cigarettes/day), and 3 months earlier had a partial resection of a right lateral leukoplakia in the anterior floor of the mouth. Histological diagnosis was moderate dysplasia.
In the examination of the oral cavity, an ulcer of approximately 10 x 5mm was observed located in the right lateral sector of the anterior floor of the mouth, adjacent to the mandible.
Palpation revealed a slight induration in the right anterior and lateral sector of the floor of the mouth, and the neck palpation was normal.
The panoramic X-ray of the jaw and the computed tomography performed in another hospital did not diagnose bone involvement (Figures 1-5).

The leukoplakia was completely resected and the histological diagnosis was moderately differentiated squamous cell carcinoma.
Contrast-enhanced tomography (CT) of the neck showed a tumor in the floor of the mouth with thickening of the mandibular periosteum and cortical irregularity of the inner margin of the right anterior sector of the mandible.
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
No pathological adenopathies were detected. The chest, abdomen and pelvis CT were normal.
The squamous cell carcinoma was staged T1 N0 M0.
A selective supraomohyoid neck dissection was performed (resection of lymph node levels I, II, III), preserving the facial artery.
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
By transoral approach the tumor was resected and a marginal mandibulotomy was performed (the inner half of the mandible was resected). In depth the sublingual gland and partially the mylohyoid muscle were resected.
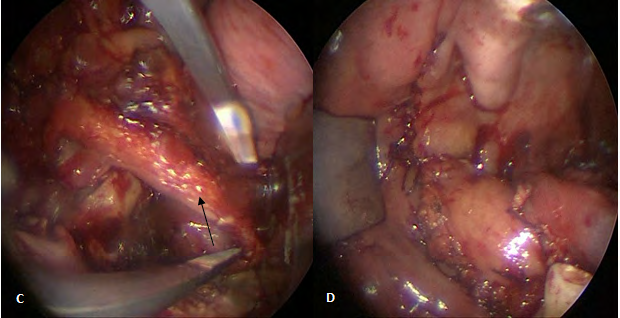
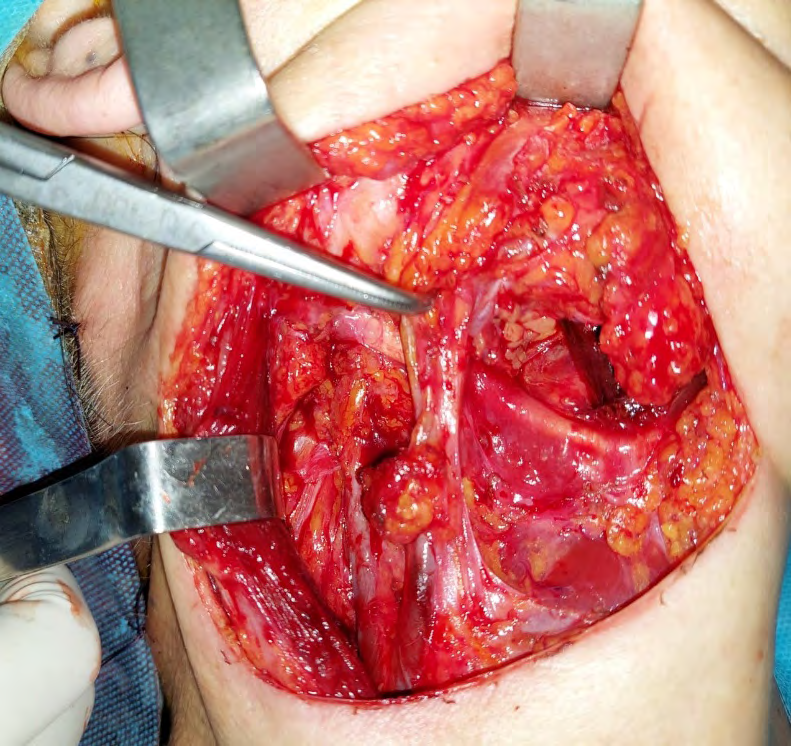
A: defect in the anterior floor of the mouth and gingiva after tumor resection and marginal mandibulotomy, B, C: dissection of the buccinator flap, D: suture of the flap to the defect, E: view of the buccinator myomucosal flap in the postoperative period.
Intraoperative biopsies of the margins were negative for carcinoma. The resulting defect was approximately 2.5cm anteroposteriorly and 1.5cm horizontally more 1cm at the level of the lower gingiva.
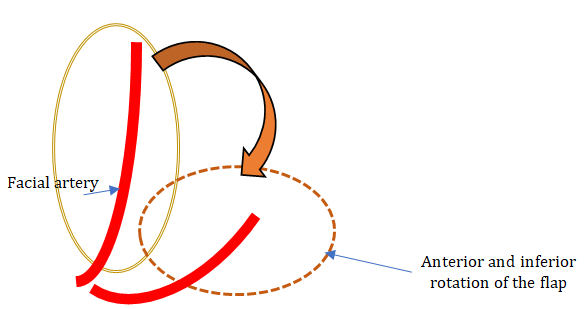
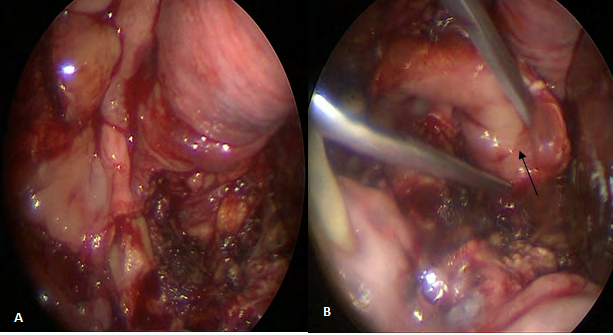
A muscular and mucosal buccinator flap was dissected through the endo-oral approach with an anterior and inferior pedicle based on the facial artery. The flap was rotated medially and inferiorly to repair the defect in the floor of the mouth and cover the exposed gingival bone left after the marginal mandibulotomy.
It was sutured with absorbable material. The patient remained hospitalized for 5 days, eating a soft diet orally. The pathological anatomy report was: lymph nodes and submandibular gland negative for neoplastic cells and squamous cell carcinoma in the surgical piece with a DOI of 1mm. The mandibular bone and margins were not affected by carcinoma.
The patient evolved well, she only had a small dehiscence in the anterior sector of the flap suture to the anterior gingiva, which healed spontaneously.
Discussion
The buccinator muscular and mucosal flap is a good option to reconstruct small and medium defects in the oral cavity.
It provides mucosal coverage similar to that of the oral cavity and also volume for the muscular part, which for example, makes it possible to reconstruct the lateral portion of the tongue.
The flap has three vascular pedicles: the facial artery, the buccal artery and the posterosuperior alveolar artery, branches of the internal maxillary artery that allow the dissection of flaps with different arcs of rotation.
The facial artery gives off posterior buccal branches that anastomose with buccal branches of the internal maxillary artery.
The venous drainage is produced by several veins that arise from the lateral aspect of the BMF to form the buccal venous plexus in the posterior part of the muscle. This plexus drains to the facial vein through 2 to 4 tributary veins and also to the pterygoid venous plexus and the internal maxillary vein through the buccal vein. The facial vein drains into the internal jugular vein through the common facial vein, but sometimes the VF drains directly into the external jugular vein or the anterior jugular vein [1].
The innervation of the BMF comes from the temporal and cervical branches of the facial nerve. Both branches converge near the buccal fat to form the buccal plexus.
When dissecting the flap, care must be taken with the opening of Stensen’s duct (mark the flap 0.5 cm below). The incision is made by cutting the mucosa and muscle until reaching the fatty plane.
The flap can be dissected with an anterior and inferior pedicle based on the facial vessels [2] (axial myomucosal flap based on the facial artery and Zhao flap [3]).
By rotating the flap, defects in the floor of the mouth (as in our case) or in the lower lip can be repaired. In general, the section of the pedicle is not necessary, but if it were, 21 days must be waited.
When performing ipsilateral neck dissections, the facial vessels should be preserved by dissecting the celluloganglionic tissue without ligating the facial artery or vein.
If it is necessary to reconstruct only the floor of the mouth without performing a marginal mandibulotomy, the flap and the vascular pedicle can be dissected down to the neck and reintroduced into the oral cavity by means of a dissection of the mylohyoid muscle.
Another possibility is to dissect a flap with a posterior pedicle (buccal artery) from the corner of the lips to the pterygoid raphe (Bozola flap). The arc of rotation of this flap allows to repair defects in the palate and the lateral pharyngeal wall.
The other variant is to dissect it with a superior pedicle based on the buccal branches of the internal maxillary artery that anastomose with the posterior buccal branches of the facial artery (retrograde flow), for which the facial artery must be ligated inferiorly.
The flap can reach the orbit through a tunnel under the skin of the infraorbital region to reconstruct the conjunctiva of the lower eyelid or the orbit. It can also be used in the reconstruction of defects of the hard palate, maxillary sinus, nasal cavity, nasal septum and upper lip.
The donor area of the flap is usually closed directly if the width is less than 3cm, in larger defects the Bichat ball fat can be used for closure.
In a study Sumarroca A, et al. [4] they reported the reconstruction of defects in 20 patients with 25 buccinator flaps. In 5 bilateral flaps were dissected simultaneously.
In 8 patients reconstructions were made due to defects in the floor of the mouth (40%), in 4 due to defects in other sectors of the oral cavity (20%), in 4 by to osteonecrosis of the jaw, in 3 by oroantral fistula (15%), and in one by postsurgical ankyloglossia (5%). In 23 patients the reconstruction was satisfactory (92%).
Necrosis of a flap occurred and another patient had a dehiscence with exposure of the underlying bone All patients had satisfactory intake and oral function.
Díaz MP, et al. [5] reported 25 patients reconstructed with a buccinator flap with an inferior or superior pedicle.
The mean size of the flaps was 41mm x 31mm and in 4 the facial pedicle was dissected up to the neck to obtain a longer flap. In 3 cases another reconstructive technique was used concomitantly. All flaps were vital.
Sixty-one patients had a facial artery-based axial flap reconstruction for defects in the floor of the mouth. In 15 there was partial necrosis, in 14 at the tip of the flap and in one at the base after sectioning the pedicle, there was no total necrosis.
Tongue mobility was satisfactory in 87% of patients [5]. In another study Ayad T, et al. [6, 7] they reported the reconstruction of partial defects of the tongue with a buccinator myomucosal flap with a posterior pedicle (buccal artery). Two patients had a distal partial necrosis of the flap (30%), which did not affect function when healed. Between 3 and 4 weeks later, the pedicle was sectioned and the flap was remodeled.
Conclusion
The buccinator myomucosal flap is an excellent option for reconstructing small and moderate-sized defects located in the oral cavity.
The flap tissue is similar to the mucosa of the mouth and is within the surgical field, the donor area can be closed without difficulty.
We declare no conflicts of interest.
References
-
Van Lierop A, Fagan JJ (2008) Buccinator myomucosal flap: Clinical results and review of anatomy, surgical technique and applications. J Laryngol Otol 122: 181- 187.
-
Bianchi B, Ferri A, Ferrari S, Copelli C, ESesenna E (2009) Myomucosal cheek flaps: applications in intraoral reconstruction using three different techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108(3): 353-359.
-
Zhao Z, Li S, Yan Y (1999) New buccinator myomucosal island flap: anatomic study and clinical application. Plast Reconstr Surg 104: 55-64.
-
Sumarroca A, Rodríguez-Bauzà E, Vega C, Fernández M, Masià J (2015) Reconstrucción de defectos de cavidad oral con colgajos tipo FAMM (colgajo músculo- mucoso de arteria facial). Nuestra experiencia. Acta Otorrinolaringológica Española 66(5): 275-280.
-
Martos Díaz P, Plasencia Delgado J, Altura Guillén O, Rodríguez Caballero B, Serrano Alvarez A, et al. (2016) Versatilidad del colgajo miomucoso de buccinador en la reconstrucción de defectos en el área maxilofacial. Rev Esp Cir Oral Maxilofac 39(1).
-
Ayad T, Kolb F, de Monés E, Mamelle G, Temam S (2008) Reconstruction of floor of mouth defects by the facial artery musculo-mucosal flap following cancer ablation. Head Neck 30: 437-445.
-
Bardazzi A, Anna Beltramini G, Autelitano L, Bazzacchi R, Rabbiosi D, et al. (2017) Use of Buccinator Myomucosal Flap in Tongue Reconstruction. The Journal of Craniofacial Surgery 28(4): 1084-1087.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?