Maxillary Sinus Barotrauma in a Silent Maxillary Sinus Syndrome Scenario: Case Report
Barosinusitis is defined as an entity where damage to a paranasal sinus occurs secondary to sudden changes in atmospheric pressure. These dysbarisms respond to Boyle's Law where -given constant temperature- the pressure of a gas is inversely proportional to its volume. On the other hand, silent sinus syndrome is a pathology with few case reports in which the paranasal sinus undergoes a remodeling of its bony walls generating, in the case of the maxillary sinus, a descent of the eyeball and a herniation of the fat of the pterygopalatine fossa. The symptoms in these patients are insidious, so the diagnosis is usually fortuitous. The authors report a case where a diagnosis of silent maxillary sinus syndrome was made after an episode of severe maxillary barosinusitis.
Introduction
Dysbarisms are all the pathophysiological phenomena that the human body can suffer as a result of the effects of changes suffered by gases in the body when subjected to variations in barometric pressure. The severity of the dysbarisms is radically different depending on the affected area.
To understand the pathophysiology of these nosological entities, it is necessary to remember Boyle’s Law, which refers to the volume expansion or contraction suffered by gases, when subjected to pressure variations, in an inverse relationship. As the pressure of a gas decreases, it tends to increase its volume and vice versa. This scenario acquires real importance in aviation, by subjecting the gases trapped in organic cavities, whether rigid or not. Being able to diffuse freely, gases will apply mechanical pressure variations on the structures that contain them.
Whenever a patient travels with a cold of the upper airways symptomatically made up of rhinorrhoea, ventilatory failure, pharyngodynia, and otalgia, the regulatory mechanisms of the auditory tube will be reduced by local inflammation. This scenario does not have major repercussions other than lack of smell, feeling of nose and ears covered and sneezing as long as the patient is on ground level. At a height of ten thousand meters, the panorama is different. Following Boyle Mariotte’s law, this crew member could be subjected to clinically significant changes during the descent where the atmospheric pressure gradually increases.
With an immobile Eustachian tube due to inflammation, the volume of oxygen in the middle ear would gradually decrease due to absorption in the mucosal capillaries, without replacement [1, 2, 3, 4, 5, 6, 7, 8, 9]. In turn, the increasing atmospheric pressure transmitted through the external auditory canal would generate a protrusion of the tympanic membrane over the middle ear [10, 11]. The sum of both will make an increase in the negative pressure of the ear causing the extravasation of liquid to it, promptly a transudate. The increase in volume of liquid, without having an escape site, would generate significant localized pain that can be disabling and cause sudden disability in flight [12]. Barotrauma is understood as the injury generated in cavities of the body that have gaseous content and that suffer a volumetric variation of the same. Some examples of barotrauma are barosinusitis, barotitis, barogastralgia, barodontalgia, among others [13, 14, 15].
On the other hand, the initial description of silent sinus syndrome (SSS) dates back to 1964 by Montgomery, et al. [16] where they reported the presence of a maxillary sinus mucocele that caused enophthalmos due to blockage of the ostiomeatal complex. However, the term was coined thirty years later, in 1994, by Soparkar, et al. [17]. This makes this entity a relatively recent pathology. Among the clinical manifestations there is the presence of spontaneous enophthalmos, understood as the displacement of the eyeball towards the posterior aspect of the orbit in the absence of traumatism or space-occupying pathology that justifies it. On the other hand, patients with SSS present hypoglobus, that is, lowering of the eyeball secondary to sinking of the orbital floor. The preceding signs generate a facial asymmetry that often makes up the only manifestation of the disease. Sinus symptoms are usually absent, a condition that gives the entity the silent condition.
The association between barosinusitis and silent maxillary sinus syndrome has not yet been described.
A case report of a patient with both morbidities is presented.
Case Report
This is a 27-year-old male patient who, during a domestic flight from the city of Buenos Aires to the city of Comodoro Rivadavia, in southern Argentina, experienced an intense left-sided headache. The pain was exquisite in the V2 innervation territory of the trigeminal nerve, with pain at the left infraorbital level and in the gums. This was triggered by an abrupt descent from approximately 30,000 feet under conditions of previous severe nasal congestion. The pain was classified as intensity 10/10 and only subsided after an intramuscular injection of glucocorticoids.
Once returned from the destination, the patient consulted our Otorhinolaryngology service where a Cone Beam CT was ordered.
A complete tomography of the craniofacial mass was performed, showing total occupation of the left maxillary sinus with atelectasis of the uncinate process, descent of the orbital floor towards the lumen of the maxillary sinus, as well as protrusion of the posterior wall of the sinus with herniation of the fat from the pterygopalatine fossa Figures 1 & 2.


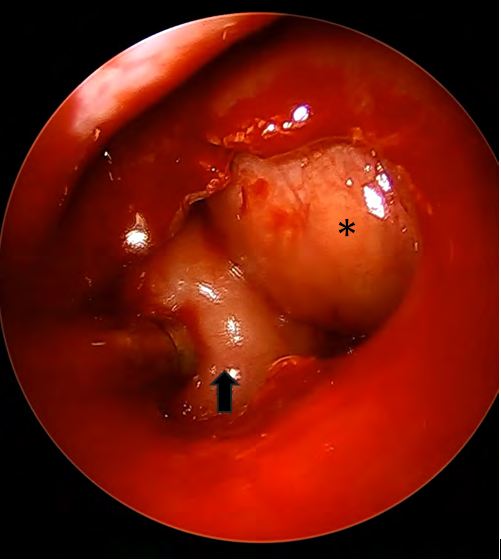
Both the nostril and the infratemporal and pterygomaxillary fossae were free of space-occupying pathology. Clinically, and retrospectively, the patient reported recurrent predominantly left frontal headaches without posterior nasal discharge or positive sinus points. In the visual aspect, he did not manifest the presence of vertical diplopia. Regarding the aesthetic aspect, sinking was found in the left maxillary region and hypoglobus with marking of the palpebral furrows after the diagnosis and the deliberate search for these signs. Therefore, the disease was silent and discovered incidentally before giving visual symptoms. Surgical treatment was decided by nasal endoscopic surgery without orbital time. To perform this, an incision was made in the lateral nasal wall with a red tip in a safe place in the middle meatus between the lacrimal eminence and the presumed location of the atelectatic uncinate process. Subsequently, the mucosa was removed with a decolating cannula before entering the maxillary sinus. Initially, a serous secretion was suctioned, which became purulent after mucosal removal. A wide median antrostomy was performed, showing both orbital and posterior wall herniations confirmed by tomography Figure 3. Finally, a polypoid degeneration of the head of the ipsilateral middle turbinate was resected and the sphenopalatine artery was located behind the ethmoid crest and cauterized. The patient was discharged on the same day, without nasal tamponade.
Discussion
The paranasal sinuses are not exempt from suffering morbid alterations when facing changes in atmospheric pressure. An analogy could be established, for example, between the middle ear and its guaranteed ventilation through the Eustachian tube. The maxillary sinus ventilation its guaranteed ventilation through its drainage ostium located in the lower third of the hiatus semilunaris. Any pathology that obliterates the sinus drainage orifice, as well as the auditory tube, could cause pathology in the corresponding cavity.
Barosinusitis can occur at any stage of flight but predominates during descent. The most affected patients are those with inflammation of the nasal mucosa (allergic rhinitis, nasal polyposis) or anatomical alterations (bullous middle turbinates, septal deviation, etc.). Two types of barosinusitis must be distinguished: sinus squeeze and sinus reverse squeeze.
The most frequently compromised paranasal sinus is the frontal sinus in 70 to 80% of cases. The maxillary sinus is affected in 19 to 29% and less frequently the ethmoid and sphenoid. Pain is the cardinal symptom and is unilateral in 85% of cases.
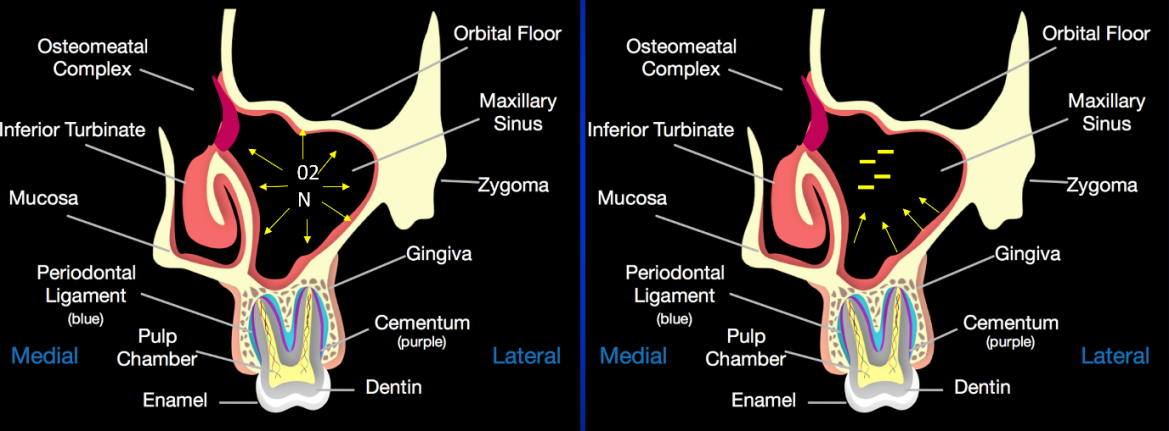
In barosinusitis with reverse squeeze phenomenon, the alteration occurs more frequently in ascent. In a patient with a bullous middle turbinate blocking the ostiomeatal complex, for example, who undergoes a rapid ascent (hence a rapid drop in atmospheric pressure), the pressure in the nasal fossa becomes negative relative to that in the maxillary sinus. The morbid alteration of the drainage ostium prevents the positive pressure of the maxillary sinus from being released to equalize with that of the nasal fossa. This generates an expansive effect within the sinus that ends up generating a medialization of the intersinus nasal wall with intense pain and epistaxis.
In barosinusitis with squeeze phenomenon Figure 4 (the most frequent of the variants), the pathology is observed more during the descent. Like the other type, morbid alterations in the nostril must coexist. As the plane descends, the atmospheric pressure increases and therefore the pressure in the nostril. If the ostium is blocked, this pressure cannot be transmitted within the paranasal sinus, leaving the latter with negative pressure with respect to the nostril. Like the plunger of a syringe withdrawing, a negative pressure is generated in the sinus that causes edema and exudate of the mucosa with pain and epistaxis to a greater extent than the reverse squeeze variant. The pain can be of great magnitude, being erroneously attributed by the patient to a dental piece. Differential diagnosis should be made with barodontalgia and trigeminal neuralgia.
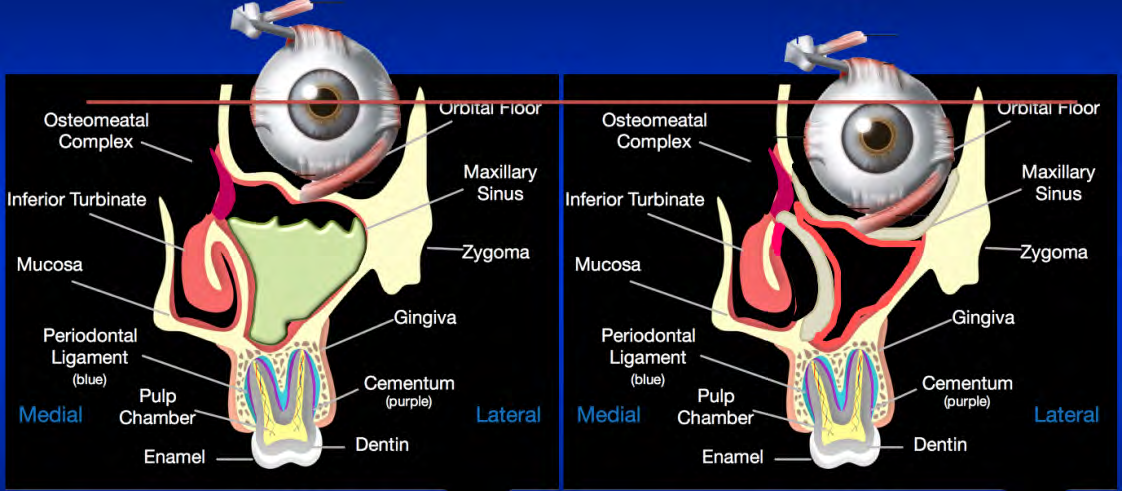
As for the Silent Maxillary Sinus Syndrome, it is known that there is some process that ends up blocking the drainage ostium of the sinus. The most common finding is atelectasis of the uncinate process. This causes the gases located within the maxillary sinus to be gradually reabsorbed into the capillaries without their renewal, generating a microclimate where negative pressure predominates.
Prolonged over time, it is the same pressure that initially causes a transudate that can become an exudate superinfected with anaerobes who take advantage of the low partial pressure of oxygen. In this way, we obtain a maxillary sinus that does not ventilate, that is occupied and that, due to the same negative pressure, generates atelectasis of the previously listed walls. As these events overlap so much in time, patients generally do not manifest rhinosinusal symptoms. Thus, the most important symptom is produced: descent of the orbital floor with diplopia in the vertical plane eventually and facial asymmetry Figure 5.
In the original description, Soparkar, et al. [17] reported 14 cases of patients with spontaneous enophthalmos associated with unilateral hypoglobus in the absence of sinus symptoms. There was no predominance of one sex over another and the average age of onset was 37 years [18, 19, 20]. On average, the progression of enophthalmos to diagnosis was 3 months (range 10 days to 2 years). This disparity in the time of evolution can trigger an inadvertent progression by the patient himself, being a relative who notices the facial asymmetry. On average, the hypoglobus manifested as a lowering of the orbital floor and consequent eyeball of about 3 to 4mm compared to the healthy contralateral eye. Enophthalmos, understood as the sinking of the eyeball posteriorly, was on average 4mm.
Nama, et al. [21] present one of the largest series, with 84 reports. In their manuscript, they detail the most widely accepted pathophysiology behind silent sinus syndrome [22, 23, 24]. It would be a blockade of the ostiomeatal complex as a trigger of atelectatic events and bone resorption in the maxillary sinus [25]. The ostiomeatal complex is the final common pathway by which the frontal, maxillary, and anterior ethmoid sinuses drain their secretions and are ventilated. This complex is made up of the uncinate process, the ethmoidal infundibulum, the ethmoid bulla, and finally, the hiatus semilunaris [26, 27].
Any morbid alteration that causes a blockage in its circulation will directly affect the paranasal sinuses involved [28, 29]. Among the pathologies that can generate a blockage are the paradoxical middle turbinate, the bullous middle turbinate, Haller’s infraorbital cells, septal deviations, and atelectasis of the uncinate process. The latter has been attributed to the genesis of the silent sinus syndrome [30].
As described, both entities are well demarcated. However, there is no such association in the consulted literature. The presence of a silent sinus syndrome predisposes to barosinusitis if the right conditions are met. As the bony walls of the maxillary sinus are weakened, we believe that the sinus pain caused by the infraorbital nerve is much higher than that found in normal situations.
Conclusion
The silent sinus syndrome, honoring the coined term, presents as main symptoms enophthalmos, hypoglobus and facial asymmetry in the absence of rhinosinusal symptoms. Its diagnosis can be delayed for long periods of time given the overlapping of its clinical evolution. Due to the negative pressure inside, the maxillary sinus suffers a volumetric reduction at the expense of atelectasis of the walls that comprise it. Radiologically, the most frequent findings are described. Regarding the treatment, it can be in one or two surgical times. Median antrostomy using an endoscopic approach is the undisputed treatment. Plastic surgery of the orbital floor may or may not be associated with different reconstruction materials.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?