Epidemiological and Etiological Aspects of Hearing Impairment in Patients at the Renaissance University Hospital in N'Djamena, Chad
Background: Hearing impairment is a common disability affecting approximately 360 million people worldwide, with around 75% of cases occurring in developing countries. The causes of this condition are diverse. Objectives: To determine the prevalence, describe the socioprofessional profile and identify the main etiologies of patients with hearing impairment in a tertiary care hospital in N'Djamena, Chad. Method: This was a prospective cross-sectional study, conducted from November 1st, 2020 to October 31st, 2021 at the ENT and Head and Neck Surgery Department of the Renaissance University Hospital in N'Djaména, Chad. All patients, aged 6 years and above that were consulted for hearing impairment, were included. They were all submitted to a clinical and audiometric examination. Results: This study ascertained the hospital prevalence of 22.5%. The sex ratio (male/female) was 3.08. The median age of patients was 35 years with an age range of 7 to 90 years. Students accounted for 24.4% of the cases. Conductive hearing loss was noted in 46.8%, sensorineural hearing loss in 37.2% and mixed hearing loss in 16% of the study population. Regarding the etiology, chronic suppurative otitis media was observed in 24.5% of the patients, presbycusis in 12.8%, seromucous otitis media in 11.7%, acoustic trauma in 10.6% and head trauma in 9.6%. Conclusion: Hearing impairment is common in ENT consultations. Most causes are due to chronic otitis media, trauma and aging. There are many preventable causes, therefore, the health care system capacity must be scaled up to address growing needs, particularly in low-income settings, which should prompt health policy makers to take appropriate action.
Introduction
Hearing impairment is the most common sensory disability in the world and is a condition of growing concern [1]. It affects nearly 360 million people worldwide (5.3% of the world’s population) and the majority of cases live in developing countries [2]. Hearing represents the main source for acquisition of language and speaking skills especially during childhood. The hearing-impaired individual is deprived of sound stimulation, and consequently, might present with emotional, social and linguistic disabilities. Therefore, it is of utmost relevance to learn about the epidemiological and etiological factors that cause auditory damage. The causes attributed to hearing loss are many and varied [3, 4, 5, 6]. The main causes include infections/diseases, age-related factors and occupational factors [7]. In sub-Saharan Africa, the prevalence of hearing impairment; defined as hearing loss > 35 dB was estimated to be 15.7% in adults over 15 years of age and 1.9% in children aged 5-14 years [8]. These estimates are based on very few African studies, including school-based hearing screenings. As for the causes, most of them are considered preventable [6]. Certain causes that can lead to hearing loss are defined as preventable and treatable conditions such as middle ear infections leading to conductive hearing loss, infectious diseases leading to sensorineural hearing loss, ototoxicity of drugs and occupational noise exposure.
In Chad, there has never been any national records, systemic scientific assessment of published, publicly available and contributed data, surveys or hospital studies on the prevalence and causes of hearing impairment. This study was conducted to determine the prevalence, describe the socio- professional profile of patients with hearing loss and identify the main etiologies in the Renaissance University Hospital in N’Djamena. In the context of a general lack of epidemiological and etiological data on hearing loss, this hospital study could provide essential data for the development of strategic plans for the management of hearing loss in a sub-Saharan African country.
Materials and Methods
This was a prospective cross-sectional study, conducted from November 1st, 2020 to October 31st, 2021, at the ENT and Head and Neck Surgery Department of the Renaissance University Hospital in N’Djamena, Chad. All patients aged 6 years and above that came for consultation for hearing loss were included. Patients under 6 years of age, known and documented psychiatric disorders, active substance abuse, who could not be expected to have the ability to follow the instructions in a relaxation training and cognitive deficits were excluded. For each patient, a clinical consultation, general physical examination, otoscopy and audiometry was performed. In case of doubt about the etiological diagnosis, the examination was completed by a computed tomography (CT) scan and/or magnetic resonance imaging (MRI) of the petrous temporal bone. Data were collected on pre-established forms including epidemiological parameters (age, sex, occupation), patient’s medical history, exposure to high levels of noise, clinical and audiometric data and the results of the medical imaging. Linear tone audiometry was performed using a Model AC50-D® audiometer in a Puma® Model PRO 25 soundproof booth. The average hearing loss in each ear was calculated by dividing the sum of the measured deficits in decibels (dB) at the frequencies of 500, 1000, 2000 and 4000 Hz by 4. The World Health Organization’s criterion was used to classify the severity of hearing loss for each ear as mild (26 to 40 dB), moderate (41 to 60 dB in adults and 31 to 60 dB in children under 15 years of age), severe (61 to 80 dB) or profound (81 to 120 dB). Above 120 dB nothing is perceived and therefore causes total deafness or cophosis. In cases where the classification of the severity of hearing loss differed between two ears, the severity of the bilateral hearing loss was based on the better ear.
The data were analyzed using SPSS version 26.0. Descriptive frequency statistics and cross-tabulations were performed. The chi-square test was used for comparison of the different proportions. A p-value of less than 0.05 is considered significant. All patients had given a verbal consent to participate in the study and to have their data published. In the case of children, a parental consent was obtained. The study was authorized by the Faculty of Human Health Sciences in N’Djamena. The study has complied with the 2013 Declaration of Helsinki.
Results
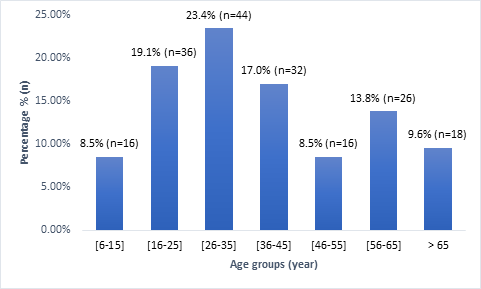
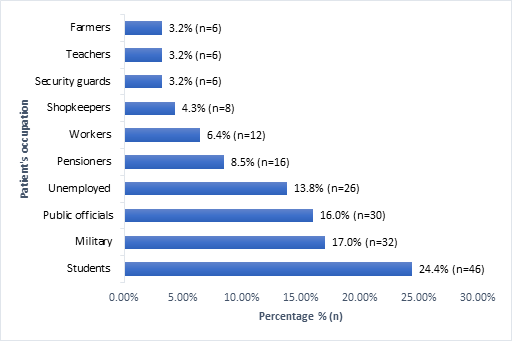
During the study period,188 patients had presented with hearing loss out of a total of 836 patients seen in ENT consultations, i.e., a hospital prevalence of 22.5%. Males accounted for 75.5% (n=142) or a sex ratio (male/female) of 3.08. The median age was 35 years with an age range of 7 to 90 years. The distribution of patients by age group is shown in (Figure 1).
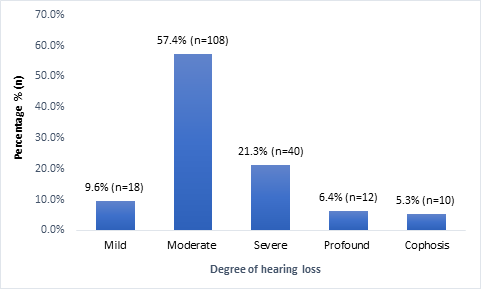
Unilateral hearing loss was observed in 51.1% of cases (n=96) and bilateral hearing loss in 48.9% of cases (n=92). Conductive hearing loss was noted in 46.8% (n=88) of the patients, sensorineural hearing loss in 37.2% (n=70) and mixed hearing loss in 16% (n=30) (Table 1). The hearing loss was moderate in 57.4% (n=108) of the patients. Figure 3 shows the degree of hearing loss.
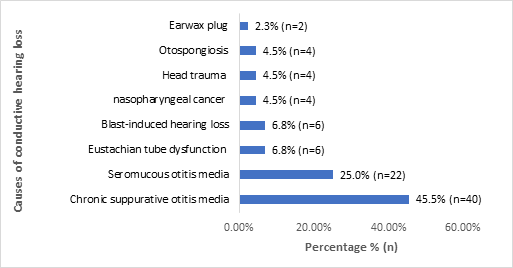
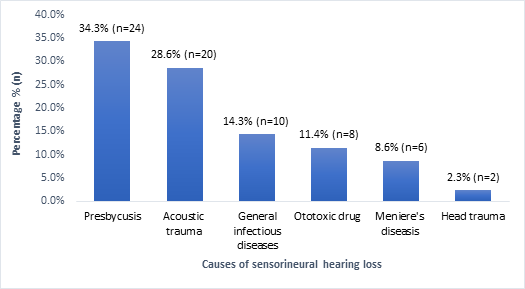
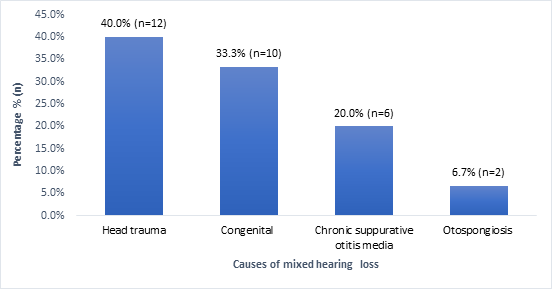
Regarding the etiology, chronic suppurative otitis media was observed in 24.5% (n=46) of the patients, presbycusis in 12.8% (n=24), seromucous otitis media in 11.7% (n=22), acoustic trauma in 10.6% (n=20) and head trauma in 9.6% (n=18). Table 2 provides a complete list of etiologies of hearing loss and their frequencies. According to the type of hearing loss, the main causes of conductive hearing loss were chronic suppurative otitis media (45.5%) and seromucous otitis media (25.0%), the main causes of sensorineural hearing loss were presbycusis (34.3%) and acoustic trauma (28.6%), and the main causes of mixed hearing loss were head trauma (40.0%) and congenital deafness (33.3%). Figures 4-6 provide information on the different etiologies of conductive, sensorineural and mixed hearing loss. The etiologies of hearing loss in our patients were associated with age (p < 10-3), occupation (p < 10-3) and degree of hearing loss (p < 10-3). Further details are given in Tables 3-5.
| Side reached | n | % | |
|---|---|---|---|
| Conductive hearing loss | Right | 34 | 18.1 |
| Conductive hearing loss | Left | 32 | 17 |
| Conductive hearing loss | Bilateral | 22 | 11.7 |
| Total | 88 | 46.8 | |
| Sensorineural hearing loss | Right | 2 | 1.1 |
| Sensorineural hearing loss | Left | 16 | 8.5 |
| Sensorineural hearing loss | Bilateral | 52 | 27.7 |
| Total | 70 | 37.2 | |
| Mixed hearing loss | Right | 4 | 2.1 |
| Mixed hearing loss | Left | 8 | 4.3 |
| Mixed hearing loss | Bilateral | 18 | 9.6 |
| Total | 30 | 16 | |
| Totals | 188 | 100 |
Table 1: Distribution of patients by the type of hearing loss.
| Etiologies | n | % |
|---|---|---|
| chronic suppurative otitis media | 46 | 24.5 |
| Presbycusis | 24 | 12.8 |
| seromucous otitis media | 22 | 11.7 |
| Acoustic trauma* | 20 | 10.6 |
| Head trauma | 18 | 9.6 |
| Congenital | 10 | 5.3 |
| General infectious diseases** | 10 | 5.3 |
| Ototoxic drug | 8 | 4.3 |
| Eustachian tube dysfunction | 6 | 3.2 |
| Blast-induced hearing loss | 6 | 3.2 |
| Otospongiosis | 6 | 3.2 |
| Meniere’s diseasis | 6 | 3.2 |
| Nasopharyngeal cancer | 4 | 2.1 |
| Earwax plug | 2 | 1.1 |
| Total | 188 | 100 |
Table 2: Distribution of cases according to the etiology of hearing impairment.
*Acute acoustic trauma (n=14; 7.4%); chronic acoustic trauma (n=6; 3.2%); **Meningitis (n=4; 2.1%); chicken pox (n=4; 2.1%); rubeola (n=2; 1.1%). Table 2: Distribution of cases according to the etiology of hearing impairment.
| Etiologies of hearing loss | Age groups (Year) | |||||||
|---|---|---|---|---|---|---|---|---|
| [6 – 15] | [16 – 25] | [26 – 35] | [36 – 45] | [46 – 55] | [56 – 65] | > 65 | Total | |
| Inflammatory and/or infectious disease | 16 | 14 | 18 | 16 | 10 | 8 | 2 | 84 |
| Traumatic injury | 0 | 10 | 16 | 6 | 6 | 4 | 2 | 44 |
| Presbycusis | 0 | 0 | 0 | 0 | 0 | 10 | 14 | 24 |
| Congenital and/or hereditary condition | 0 | 10 | 6 | 0 | 0 | 0 | 0 | 16 |
| Ototoxic drug | 0 | 2 | 0 | 4 | 0 | 2 | 0 | 8 |
| Meniere’s disease | 0 | 0 | 2 | 4 | 0 | 0 | 0 | 6 |
| Nasopharyngeal cancer | 0 | 0 | 2 | 0 | 0 | 2 | 0 | 4 |
| Earwax plug | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 2 |
| Total | 16 | 36 | 44 | 32 | 16 | 26 | 18 | 188 |
Table 3: Etiologies of hearing impairment according to age groups.
Χ2 = 93,262 ; ddl=42 ; p < 10-3. Table 3: Etiologies of hearing impairment according to age groups.
| Occupation | Etiologies of hearing loss | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Inflammatory/ infectious disease | Traumatic injury | Pres bycusis | Congenital and/ or hereditary condition | Ototoxic drug | Meniere’s disease | Nasophary ngeal cancer | Earwax plug | Total | |
| Students | 30 | 2 | 0 | 10 | 2 | 0 | 2 | 0 | 46 |
| Military | 4 | 28 | 0 | 0 | 0 | 0 | 0 | 0 | 32 |
| Public officials | 16 | 4 | 4 | 2 | 0 | 2 | 2 | 0 | 30 |
| Unemployed | 12 | 6 | 0 | 4 | 2 | 2 | 0 | 0 | 26 |
| Pensioners | 2 | 2 | 12 | 0 | 0 | 0 | 0 | 0 | 16 |
| Workers | 8 | 0 | 0 | 0 | 0 | 2 | 0 | 2 | 12 |
| Shopkeepers | 0 | 2 | 6 | 0 | 0 | 0 | 0 | 0 | 8 |
| Teachers | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 |
| Security guards | 4 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 6 |
| Farmers | 2 | 0 | 2 | 0 | 2 | 0 | 0 | 0 | 6 |
| Total | 84 | 44 | 24 | 16 | 8 | 6 | 4 | 2 | 188 |
Table 4: Etiologies of hearing impairment according to the patient’s occupation.
Χ2 = 142,926 ; ddl=63 ; p < 10-3. Table 4: Etiologies of hearing impairment according to the patient’s occupation.
| Etiologies of hearing impairment | Degree of hearing loss | |||||
|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | Profound | Cophosis | Total | |
| Inflammatory/infectious disease | 12 | 60 | 8 | 2 | 2 | 84 |
| Traumatic injury | 4 | 18 | 14 | 8 | 0 | 44 |
| Presbycusis | 0 | 14 | 8 | 2 | 0 | 24 |
| Congenital and/or hereditary condition | 0 | 6 | 10 | 0 | 0 | 16 |
| Ototoxic drug | 0 | 2 | 0 | 0 | 6 | 8 |
| Meniere’s disease | 0 | 4 | 0 | 0 | 2 | 6 |
| Nasopharyngeal cancer | 0 | 4 | 0 | 0 | 0 | 4 |
| Earwax plug | 2 | 0 | 0 | 0 | 0 | 2 |
| Total | 18 | 108 | 40 | 12 | 10 | 188 |
Table 5: Etiologies of hearing loss according to the degree of hearing impairment.
Χ2 = 81,610 ; ddl=28 ; p < 10-3. Table 5: Etiologies of hearing loss according to the degree of hearing impairment.
Discussion
To our knowledge, in Chad, this is the first study done to examine the prevalence and etiologies of hearing loss in hospitals. Using a threshold of 26 dB, the prevalence of hearing loss obtained in this study was 22.5%. The prevalence of hearing impairment varies considerably between studies in sub-Saharan Africa; 3.6% in Cameroon [4], 5% in Mozambique [9], 17.5% in South Africa [10] and 18% in Uganda [11].
Several factors contribute to this variation in prevalence across studies, including the different study settings (community, school or hospital) and the threshold used to measure hearing loss. Using a low threshold such as 25 dB would identify a mild hearing loss and produce a higher prevalence, whereas a pure tone threshold of 40 dB would result in a lower prevalence where only moderate and severe hearing loss would be considered. In any case, sub-Saharan Africa remains one of the regions of developing countries where the prevalence of hearing impairment is significantly higher than in developed countries. Some available reports indicate a prevalence of 11.5%-20.3% for adults (≥ 15 years) and 1.2%-3.0% for children (5-14 years) in low-income countries compared to 4.0%-6.4% for adults (≥ 15 years) and 0.3%-0.6% for children (5-14 years) in high-income countries [12]. In the United States, the prevalence of hearing impairment is estimated to be 2.5% in people over 12 years of age [13]. The high prevalence of hearing loss in sub-Saharan Africa could be attributed to poor health systems that are not always adequately equipped to prevent, detect and manage the causes of hearing loss [14].
As for the socio-professional profile of the patients, the study showed a predominance of males (sex ratio = 3.08); students represented 24.4%, soldiers represented 17% and civil servants represented 16% of the patients. The high presence of military civilians in this series is due to the fact that our tertiary care hospital has been receiving a large number of war casualty victims of the terrorist attacks by the Boko Haram sect in the Lake Chad region for the past three years. Previous research has shown that men are more likely to have hearing difficulties than women partly due to increased exposure to ear diseases [15], noisy workplaces [16, 17], military service, and the use of firearms [18].
In this study, regarding the etiologies of hearing loss, infectious diseases were in the forefront, followed by acoustic trauma, cranial or auricular lesions; presbycusis; congenital and/or genetic conditions, and the use of ototoxic drugs. All of these conditions are widely cited in the literature but in different proportions [2, 19, 20, 21, 22, 23, 24, 25]. It is difficult to make meaningful comparisons because of variations in the methods used in different studies. However, it should be noted that, as with other studies of hearing impairment in sub-Saharan Africa, most of the causes found in this study are preventable. These include chronic suppurative otitis media, infections leading to sensorineural hearing loss, such as meningitis, measles, and chicken pox, noise exposure and drug ototoxicity. Furthermore, this study also showed that the causes of hearing loss were associated with age groups, occupation and degree of hearing loss. Infectious diseases were the only cause of deafness in children aged 6 to 15 years and the main cause in students. While in other studies, genetic conditions and abuse of ototoxic drugs were associated with infectious diseases in this age group [26, 27]. Over the age of 65, presbycusis seemed to predominate and was more prevalent in the retired group. Some authors question the causal mechanism of hearing loss in the elderly and seek to understand the link between age-related hearing loss and cognitive decline [28]. The main causes of hearing loss in the military were noise injury and acoustic blast trauma. The exposure of military personnel to noise trauma is well reported in the literature [29, 30, 31]. Drug ototoxicity was noted in patients with no or low income (students, unemployed and security guards). In our context, poverty is a source of self-medication and patients have easy access to anti-malarial drugs, aminoglycosides such as gentamycin and loop diuretics such as furosemide, thus exposing them to drug-induced ototoxicity, which is probably the most functionally dangerous cause of hearing impairment in our patients (6 out of 8 patients that were drug-induced had cophosis). The rest of the etiologies resulted in moderate to profound degrees of disabling hearing impairment with the exception of cerumen impaction, which only resulted in mild hearing loss.
Conclusion
Hearing impairment in adults and children is common at the Renaissance University Hospital in N’Djamena, Chad. It affects men more than women. The causes are dominated by infectious diseases, presbycusis and noise injury. This study reveals a large proportion of preventable hearing loss, thus, highlights the importance of maximizing efforts in primary health care services to prevent or treat preventable causes in a timely manner. There is a clear need for a population- based study at the national level to estimate the prevalence of hearing impairment in Chad.
Declarations
- Ethics Approval and Consent to Participate This study has been authorized by the Faculty of Human Health Sciences in N’Djamena (Reference n° 276/CMT/ PCMT/PMT/MESRI/SE/DGM/UNDJ/SG/FSSH/21) and has been complied with the 2013 Declaration of Helsinki. All the patients were consented to participate in the study.
- Consent for Publication A verbal consent was obtained from participants for the publication of the data.
- Competing Interests The authors have nothing to declare.
- Funding The authors did not receive support from any organizations for this study.
- Author Contributions All authors contributed to the design and development of this work. AAT was responsible for analyzing the data and writing the manuscript. The preparation of the material and data collection were carried out by BA and YAA. All authors have read and approved the final manuscript.
References
-
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (2016) Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388(10053): 1545-1602.
-
Khalifa AFM (2020) Pathological and clinical profile of hearing loss among Sudanese children attending the Khartoum Teaching Hospital. J Family Medicine Primary Care 9(6): 2720-2723.
-
Bright T, Shan X, Xu J, Liang J, Xiao B, et al. (2020) Field- testing of a rapid survey method to assess the prevalence and causes of hearing loss in Gao’an, Jiangxi province, China. Arch Public Health 78: 16.
-
Tingang EW, Noubiap JJ, F Fokouo JV, Oluwole OG, Nguefack S, et al. (2020) Hearing Impairment Overview in Africa: the Case of Cameroon. Genes (Basel) 11(2): 233.
-
James M, Kumar P, Ninan PJ (2018) A study on prevalence and risk factors of hearing impairment among newborns. Int J Contemp Pediatr 5(2): 304-309.
-
Yalcouyé A, Traoré O, Taméga A, Maïga AB, Kané F, et al. (2021) Etiologies of Childhood Hearing Impairment in Schools for the Deaf in Mali. Front Pediatr 9: 726776.
-
Mulwafu W, Kuper H, Ensink RJH (2016) Prevalence and causes of hearing impairment in Africa. Trop Med Int Health 21(2): 158-165.
-
Trott M, Smith L, Xiao T, Veronese N, Koyanagi A, et al. (2021) Hearing impairment and diverse health outcomes: An umbrella review of meta-analyses of observational studies. Wien Klin Wochenschr 133(19- 20): 1028-1041.
-
Clark JL (2008) Hearing loss in Mozambique: current data from Inhambane Province. Int J Audiol 47 (S1): 49- 56.
-
Louw C, Swanepoel W, Eikelboom RH, Hugo J (2018) Prevalence of hearing loss at primary health care clinics in South Africa. Afr Health Sci 18(2): 313-320.
-
Westerberg BD, Lee PK, Lukwago L, Zaramba S, Bubikere S, et al. (2008) Cross-sectional survey of hearing impairment and ear disease in Uganda. J Otolaryngol Head Neck Surg 37(6): 753-758.
-
Stevens G, Flaxman S, Brunskill E, Mascarenhas M, Mathers CD, et al. (2013) Global Burden of Disease Hearing Loss Expert Group. Global and regional hearing impairment prevalence: an analysis of 42 studies in 29 countries. Eur J Public Health 23(1): 146-152.
-
Goman AM, Lin FR (2016) Prevalence of Hearing Loss by Severity in the United States. Am J Public Health 106(10): 1820-1822.
-
Lebeko K, Bosch J, Noubiap JJ, Dandara C, Wonkam A (2015) Genetics of hearing loss in Africans: use of next generation sequencing is the best way forward. Pan Afr Med J 20: 383.
-
Salisu AD (2010) Otology practice in a Nigerian tertiary health institution: A 10-year review. Ann Afr Med 9(4): 218-221.
-
Glenister KM, Simmons D (2019) Hearing loss and access to audiology services in rural victoria: Findings from the crossroads study. Noise Health 21(102): 217-222.
-
Moore DR, Edmondson-Jones M, Dawes P, Fortnum H, McCormack A, et al. (2014) Relation between speech-in- noise threshold, hearing loss and cognition from 40-69 years of age. PLoS One 9(9): e107720.
-
Henderson A, Waddell A, Pearson C (2016) A review of the diagnosis and management of sudden hearing loss in the military population. J R Nav Med Serv 102(2): 110- 116.
-
Rajput MS, Rajput MSA, Arain AA, Zaidi SS, Hatem A, et al. (2020) Mucosal Type of Chronic Suppurative Otitis Media and the Long-Term Impact on Hearing Loss. Cureus 12(9): e10176.
-
Singer AEA, Abdel-Naby Awad OG, El-Kader RMA, Mohamed AR (2018) Risk factors of sensorineural hearing loss in patients with unilateral safe chronic suppurative otitis media. Am J Otolaryngol 39(2): 88-93.
-
Imam L, Hannan SA (2017) Noise-induced hearing loss: a modern epidemic?. Br J Hosp Med (Lond) 78(5): 286- 290.
-
Michels TC, Duffy MT, Rogers DJ (2019) Hearing Loss in Adults: Differential Diagnosis and Treatment. Am Fam Physician 100(2): 98-108.
-
Yang T, Guo L, Wang L, Yu X (2019) Diagnosis, Intervention, and Prevention of Genetic Hearing Loss. Adv Exp Med Biol 1130: 73-92.
-
Dillard LK, Fullerton AM, McMahon CM (2021) Ototoxic hearing loss from antimalarials: A systematic narrative review. Travel Med Infect Dis 43: 102117.
-
Guo J, Chai R, Li H, Sun S (2019) Protection of Hair Cells from Ototoxic Drug-Induced Hearing Loss. Adv Exp Med Biol 1130: 17-36.
-
Kuschke S, Swanepoel W, le Roux T, Strauss S (2020) Profile of childhood hearing loss in the Western Cape, South Africa. Int J Pediatr Otorhinolaryngol 137: 110248.
-
Osei AO, Larnyo PA, Azaglo A, Sedzro TM, Torgbenu EL (2018) Screening for hearing loss among school going children. Int J Pediatr Otorhinolaryngol 111: 7-12.
-
Uchida Y, Sugiura S, Nishita Y, Saji N, Sone M, et al. (2019) Age-related hearing loss and cognitive decline - The potential mechanisms linking the two. Auris Nasus Larynx 46(1): 1-9.
-
Moore BCJ, Von Gablenz P (2021) Sensitivity and specificity of a method for diagnosis of military noise- induced hearing loss. J Acoust Soc Am 149(1): 62.
-
Lowe DA, Moore BCJ (2021) Audiometric assessment of hearing loss sustained during military service. J Acoust Soc Am 150(2): 1030.
-
Smith C, Beamer S, Hall S, Helfer T, Kluchinsky TA (2015) A Preliminary Analysis of Noise Exposure and Medical Outcomes for Department of Defense Military Musicians. US Army Med Dep J pp: 76-82.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?