Kimura Disease: A Diagnostic Perplexity
Introduction: Kimura disease (KD) is a rare condition of unknown etiology and pathogenesis. This is more common in young males of Asian descent. The most common clinical presentation is presence of unilateral subcutaneous mass in the head and neck region, especially in post-auricular area. We present a case of KD in 26- year- old Asian man who presented with subcutaneous mass behind both auricles. Case report: A 26- year- old man presented to ORL-HNS outpatient department of tertiary care centre with chief complaint of mass behind both ear for 5 months. Incisional biopsy was performed under local anesthesia. Histopathological examination report confirmed the case as KD. Patient was managed with intralesional triamcinolone injection. Conclusion: Kimura disease, though rare, should be considered in differential diagnosis of head and neck subcutaneous masses. A high-index of suspicion and tissue biopsy confirmation is essential to diagnose this condition.
Introduction
A Japanese doctor named Kimura et al. published a systemic description of this disease and formally coined it as ‘Kimura disease’ in 1948 [1], even though the case was first reported by Kimm and Szeto in 1937 in China [2]. KD also known as eosinophilic lymphogranuloma, is a rare benign inflammatory disorder of unknown etiology. The exact cause of chronic inflammation in KD is uncertain. However, some attributed it to a hypersensitivity reaction or immune mediated response toward environmental agents [3]. The disease is characterized by the triad of painless subcutaneous masses in head and neck, blood and tissue eosinophilia, and increased serum IgE levels. Though, KD has no potential for malignant transformation, it can grow big and cause functional and cosmetic disfigurement.
A 26- year- old male patient presented to ORL-HNS outpatient department with a chief complaint of swelling behind both ears since 5 months. On examination, nodular swelling was observed in bilateral post-auricular region. The swelling was painless, slowly growing but associated with mild itchiness.
There was no history of chronic cough, night sweats, anorexia or loss of weight, so the diagnosis of pulmonary tuberculosis was excluded. On general physical examination, he had stable vital signs: his temperature was 37⁰C, heart rate of 72 bpm and respiratory rate of 16 breaths/min. Head and neck examination revealed a 2x1.5cm swelling behind right ear and 3x1.5cm swelling behind left ear. On palpation, the swelling was nodular with welldefined borders, rubbery to firm in consistency (Figures 1 & 2). Initial laboratory investigations revealed normal full blood count except a slightly higher eosinophils count of 0.5 g/dL. Serum immunoglobulin E (IgE) level was not performed for this patient.
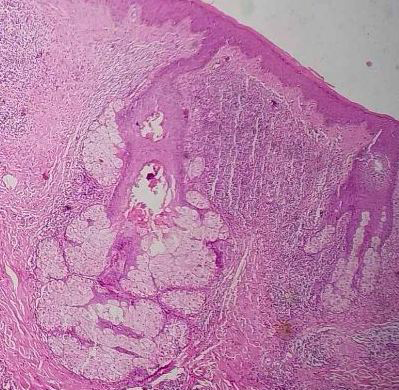
The patient was subjected to incisional biopsy and the specimen was sent for histopathological examination (HPE). HPE showed lymphoid tissue with reactive follicular hyperplasia, eosinophilic deposits within germinal centers, and mixed inflammatory infiltrate predominantly of eosinophils and confirmed diagnosis of KD was made (Figure 3). The patient was treated with intralesional triamcinolone injection 10mg/cc every 2 weeks for 3 months.


Discussion
KD is a chronic inflammatory disorder of unknown origin and benign clinical course. The exact prevalence is still undetermined, but occurs mostly in young and middle- age men originating from East Asia and South East Asia [4]. It presents as a deep, subcutaneous mass in the head and neck region and is frequently associated with regional lymphadenopathy or salivary gland involvement.
Rarity of this condition leads to diagnostic dilemma as its features are often confusing and overlap with other entities. The most common disease that resembles KD is angiolymphoid hyperplasia with eosinophilia (ALHE), both having predilection for head and neck region. However, KD is differentiated by regional lymph node involvement, the presence of lymphoid tissue with prominent germination centre and the absence of endothelial atypia. KD is predominantly lymphoid follicle disorder whilst ALHE is a vascular disorder [5]. Other differential diagnosis includes reactive lymphadenopathy, angioma/ lymphangioma/ hemangioma, lymphoma, salivary gland tumour, nodal metastases, Kikuchi disease and Mikulicz’s disease.
KD is usually a localized process without systemic symptoms. Cases with itchiness, urticaria, and chronic eczema have been reported in literature. The most significant association is renal disease, which may develop before or concurrently with KD [6]. Peripheral eosinophilia, high serum IgE, and multiple lymphadenopathies are often associated with KD. Different imaging modalities like ultrasonography/CT/MRI scans can help in delineating the extent and also in evaluating the progression of the disease. Definitive diagnosis is ascertained by tissue biopsy; fine needle aspiration cytology can be helpful in cases of recurrence. Histopathology of the subcutaneous lesions, salivary glands and lymph nodes reveals a prominent and mixed inflammatory cellular infiltrate composed mainly of eosinophils and lymphocytes. The inflammatory infiltrate contains numerous lymphoid follicles with prominent germination centres interspersed with variable degrees of fibrosis.
Surgery is the mainstay of treatment, although regional or systemic corticosteroid therapy, cytotoxic therapy, and radiation have been used [7]. Treatments for KD are usually unsatisfactory as new lesions may occur and recurrence after resection and discontinued steroid treatment is common.
Conclusion
KD, though rare, should be considered in differential diagnosis in patients with subcutaneous nodules in head and neck region, especially in young Asians males with peripheral eosinophilia and increased serum IgE. A detailed clinical history along with radiological and pathological correlation is necessary for the correct diagnosis. Treatments for KD are not satisfactory as there is high chances of recurrences following resection or withdrawal of steroid therapy. So, routine follow up is a must.
Conflict of Interest: None Funding Source: None Ethical approval: As this is a case report approval from IRB has been exempted Consent: written consent was obtained from the patient Author Contributions: Sonika Dhari Shrestha: drafting and compiling of article, getting consent from patient Arun KC:
supervision of drafting process
References
-
Kimura T, Yoshimura S, Ishikawa E (1948) On the unusual granulations combined with hyperplastic changes of lymphatic tissue. Trans Soc Pathol Jpn 37: 179-180.
-
Kim HT, Szeto C (1937) Eosinophilic hyperplastic lymphogranuloma, comparison with Mikulicz’s disease. Chin Med J 23: 670-699.
-
Hashim HZ, Hoo FK, Sazlly Lim SM, Mohamed MH, Ramachandran V, et al. (2017) Kimura disease – A case report and review of the literature. Polish Ann Med 24(1): 64-66.
-
Wang DY, Mao JH, Zhang Y, Gu WZ, Zhao SA, et al. (2009) Kimura disease: a case report and review of the Chinese literature. Nephron Clin Pract 111(1): c55-61.
-
Briggs PL (2006) Kimura disease is not angiolymphoid hyperplasia with eosinophilia : clinical and pathological correlation with literature review and definition of diagnostic criteria An Bras Dermatol 81(2): 167-173.
-
Rajpoot DK, Pahl M, Clark J (2000) Nephrotic syndrome associated with Kimura disease. Pediatr Nephrol 14(6): 486-488.
-
Day TA, Abreo F, Hoajsoe DK, Aarstad RF, Stucker FJ (1995) Treatment of Kimura’s disease: a therapeutic enigma. Otolaryngol Head Neck Surg 112(2): 333-337.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?