Effect of A Clinician-Delivered Chewing Program on Masticatory Function in Children with Cerebral Palsy
Objectives: Studies documenting the training effect of the Functional Chewing Training (FCT) program using objective methods are limited. The present study attempts to evaluate the effect of FCT on chewing dynamics by comparing the pre-, post-treatment and follow-up scores in children with cerebral palsy (CP). Study design: A time series design was employed to study the treatment effects. Methods: Six children with a confirmed diagnosis of oral dysphagia secondary to CP in the age range of 3 to 8 years formed the participant group. Chewing performance was assessed using Mastication Observation Evaluation (MOE, Remijn et al., 2014) and quantified using surface electromyography (sEMG) for the masseter muscle. Subsequently, 20 sessions of intensive chewing training was carried out. The assessments were repeated after intervention and at 4 weeks post-discharge, during which no intervention or home training was provided. Results: Friedman’s Two-Way Analysis of Variance revealed that there was a significant improvement in jaw, lip, and tongue scores for chewing as well as for the sEMG parameters. Wilcoxon Signed Rank test revealed that there was a significant difference in the pre- versus post-therapy and pre- versus follow-up conditions for all the parameters (p<0.017). Conclusions: The study revealed that FCT leads to improvements in lip seal, jaw stability and tongue lateralization aiding in effective masticatory performance. The continued improvement post-discharge indicates the effect of better management and progression of food textures. The present study is one of the first to elucidate the efficacy of the FCT program by illustrating the changes with respect to instrumental measures.
Introduction
Mastication or chewing is defined as a rhythmic oral motor activity that aids in grinding and softening solid food [1]. Chewing function has two main stages, viz. food transportation and food processing. Food transportation begins with biting the food and continues with transporting the food from the front part of the mouth to the molars by tongue. The food processing involves a series of masticatory cycles to comminute and soften the food for swallowing [2].
The development of chewing is the result of a complex interface between the developing nervous system, various physiological systems, and the environmental factors that begin in embryologic and fetal periods and continue through infancy and early childhood [3]. Chewing emerges only during the second half of the first year of life and continues to develop during childhood [4, 5]. After around 7-9 months, with the development of teeth, munching begins which involves the up and down movements of the jaw. This is followed by rotary chewing, which begins to emerge by around 12-14 months, during which the horizontal movements of the jaw appear and children learn to rotate the jaw. During this stage, children learn to handle solid foods and different textures [6].
Most children negotiate the necessary developmental sequence of chewing without significant difficulties, however, some children end up with chewing difficulties which can affect swallowing. Chewing difficulties occurring due to developmental delays are usually associated with prematurity, learning disabilities, or various neurological conditions. Cerebral palsy (CP) is one such disorder in which feeding, and specifically chewing could be impaired. Children with CP are chronically classified as malnourished due to their oral motor dysfunction, chewing deficits, and postural abnormalities [7]. Globally, the incidence of CP is estimated to be 2 per 1000 live births [8]. A study reported that in India, the incidence of CP is up to 2 to 2.5 cases per 1000 live births, making it the most common cause of disability according to the Indian Academy of Cerebral Palsy (IACP) [9].
The prevalence of chewing deficits in quadriplegic children with CP was reported to be 41% and around 26% of children with CP had deficits in chewing solid food textures [10]. A recent study found that 76% of children with spastic CP had some degree of chewing deficits [11]. In the Indian context, authors have reported that 81% of parents reported chewing difficulties in children with CP [12]. Another recent study carried out in India, reported that in 70% of the children with CP, the inability to chew food was the most persisting deficit [13]. These difficulties can affect the nutritional status, growth, general health, and quality of life of the child as well as the entire family. Therefore, it is important to treat chewing deficits in children with CP as this will have a positive impact on the physiological and emotional well-being of the child.
A few strategies have been used in the past to treat chewing deficits in children with CP, which have revealed positive outcomes such as behavioral training and oral sensorimotor training [14, 15, 16, 17, 18, 19]. However, these approaches primarily focus on the underlying impairment and do not include training the chewing function. They focus on individual oromotor skills such as tongue lateralization, lip control, and jaw strengthening, which are only prerequisites for chewing.
A relatively recent program called functional chewing training (FCT) was proposed by Arslan and colleagues for children with CP [20]. They believed in a functional approach to improve chewing, which involves training the oromotor structures for the targeted function and generalizing those functions to everyday activities. The protocol includes two domains viz., impairment-based (positioning for feeding and food placement, orosensory stimulation, and chewing exercises) and adaptive components (adjustments made to the food textures). This protocol was carried out as a home training program by them and the parents were trained about the procedure and standardized brochures related to the same were provided. The authors reported that the proposed chewing training was found to be effective in comparison to traditional oral-motor exercises.
In sum, though various strategies have been used to improve chewing, the most recent among them is FCT, which not only lays emphasis on the underlying impairment, but also focuses on generalization of the chewing behavior using food of different consistencies, thus incorporating both impairment-based and adaptive-based components. Though Arslan and colleagues have assessed the efficacy of the FCT through a randomized controlled trial, they have done it as a home program by training the parents of children with CP. During a home-based program, there could be various uncontrolled variables, like not adhering to the protocol for the recommended days or duration, lack of cooperation from the child, and other environmental and personal factors, leading to a dilution of the program at the execution level.
Hence, there is a need to assess its efficacy through a clinician-delivered program. Further, the existing studies have not studied the maintenance effect of FCT, after it is withdrawn. Studies in the field of pediatric feeding therapy and chewing therapy in particular are also essential in the Indian context as the feeding practices and foods consumed vary in comparison to the other countries. Therefore, the present study was planned to assess the effects of a clinician- delivered FCT on children with CP.
Aim and Objectives
To evaluate the effect of clinician-delivered FCT in children with CP by comparing the pre-, post-treatment, and follow-up changes in the following outcome variables: 1. Masticatory performance including jaw, lip and tongue scores, and total mastication score. 2. Masticatory efficiency including amplitude measure, duration of chew, and inter-chew duration.
Methods
A time series design was employed to study the treatment effects within the group.
Participants
Six children (4 males and 2 females) with a confirmed diagnosis of oral dysphagia secondary to CP in the age range of 3 to 8 years (mean age = 5.1 years; SD = 1.8 years) formed the participant group. All the children had difficulty chewing and consumed only pureed and moist food. Participants with a score of 3 and above were selected based on the Karaduman Chewing Performance Scale (KCPS) [21]. This scale provides the overall chewing performance level, which is rated on a scale from 0 to 4, wherein 0 indicates ‘normal chewing function’ and 4 indicates ‘no biting and chewing abilities’. The children had an IQ of at least 35-50 and were able to comprehend simple instructions. They had adequate head and neck control and appropriate dental development.
Procedure
Prior to the commencement of the training, a detailed baseline evaluation was carried out. Masticatory performance was assessed using Mastication Observation Evaluation (MOE) [22]. This tool consists of 8 items, which assesses the isolated oromotor movements of the tongue, lip, and jaw during chewing. Each item is provided a score of 1 to 4, depending on the level of functioning and a higher score indicates better functional use.
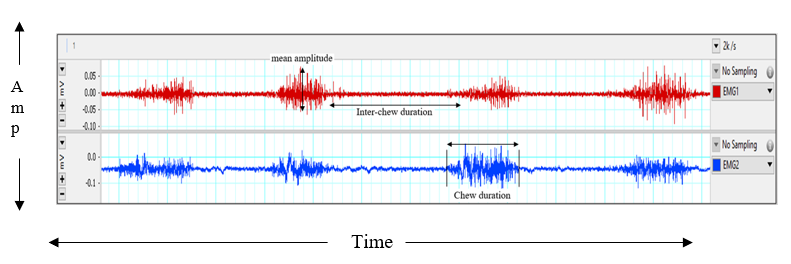
Masticatory performance was also quantified using surface electromyography (sEMG, Delsys Trigno-Power Lab 8/36) by recording the electrical signals emitted by the left and right masseter muscles while chewing a biscuit. The sEMG device contains wireless electrodes, which will pick up the electrical muscle activity and record the muscle tissue contractions, while the participant is chewing. The outcome measures recorded were mean amplitude, duration of a chew, and inter-chew duration. The waveform of the sEMG signal, which will be used to elicit the various measures has been depicted in (Figure 1) below.
The caregivers were oriented regarding the physiological aspects of chewing, the prerequisites for achieving adequate chewing abilities, the use of oromotor tools, and the importance of regular home training for the same. Before the commencement of training sessions, written consent was obtained from the caregivers and all the procedures were carried out by adhering to the guidelines of the Ethics Approval Committee for Bio-Behavioral Research of the institute (DOR.9.1/Ph.D/KV/921/2020-21 dated 10.02.2023).
Using the framework provided, the researcher in the presence of the caregiver, carried out 20 sessions of intensive FCT including impairment-based (positioning, oral sensorimotor treatment, chewing exercises) and adaptive (oromotor appliances, texture progression) activities. The caregivers were provided with the training tools and were instructed to carry out the FCT prior to every meal (at least 3 times a day). The training program included five steps such as proper seating position of the child, orosensory stimulation including massaging the gingival region, chewing exercises using chewy tubes of varying hardness, food placement using food feeders, and generalization to different food consistencies (soft, medium and hard solids). The assessments were repeated after intervention and at 4 weeks post-discharge, during which no intervention or home training was provided.
Statistical Analysis
The data obtained from the subjective and objective analyses for all participants was tabulated and appropriate statistical analysis was applied using the Statistical Package for Social Sciences Version 26.0 (SPSS). Descriptive statistics were computed to obtain the median and interquartile range for all the outcome measures. The non-parametric Friedman’s Two-Way Analysis of Variance was used to compare MOE and sEMG parameters. Pairwise comparisons between treatment timelines were carried out using Wilcoxon Signed Rank test.
Results
Friedman’s Test was used to compare MOE parameters such as jaw, lip, tongue, and overall mastication scores across pre-, post-treatment and follow-up conditions. The median values clearly indicated that there was an improvement in all the parameters across timelines. Pairwise comparisons using Wilcoxon Signed Rank test with adjusted alpha revealed that there was a significant difference in the jaw, lip, and tongue scores in the pre- versus post-therapy and pre- versus follow- up conditions. However, in the overall mastication scores there was a significant difference between all three timelines at 0.05 level of significance. The results have been depicted in Table 1 below.
| MOE scores | Median (IQR) | Friedman's test statistic X²(2) | Pairwise comparisons |Z| | ||||
|---|---|---|---|---|---|---|---|
| I-II | II-III | I-III | |||||
| Jaw score | I | 2.0 (1.25) | 11.14 | 2.23* | 1.73 | 2.33* | |
| Jaw score | II | 6.0 (1.25) | 11.14 | 2.23* | 1.73 | 2.33* | |
| Jaw score | III | 6.0 (0.5) | 11.14 | 2.23* | 1.73 | 2.33* | |
| Lip score | I | 2.0 (1.25) | 11.2 | 2.25* | 1.41 | 2.33* | |
| Lip score | II | 3.5 (1.25) | 11.2 | 2.25* | 1.41 | 2.33* | |
| Lip score | III | 4.0 (1.0) | 11.2 | 2.25* | 1.41 | 2.33* | |
| Tongue score | I | 4.5 (2.25) | 11.14 | 2.22* | 1.73 | 2.26* | |
| Tongue score | II | 9.0 (4.0) | 11.14 | 2.22* | 1.73 | 2.26* | |
| Tongue score | III | 9.5 (3.0) | 11.14 | 2.22* | 1.73 | 2.26* | |
| Total mastication score | I | 12.5 (4.75) | 12 | 2.21* | 2.23* | 2.23* | |
| Total mastication score | II | 24.5 (4.25) | 12 | 2.21* | 2.23* | 2.23* | |
| Total mastication score | III | 26.0 (4.75) | 12 | 2.21* | 2.23* | 2.23* |
Table 1: Median, Inter Quartile Range (IQR), Friedman Test Statistic And |Z| Value Across Treatment Timelines for Mastication **N
Table 1: Median, Inter Quartile Range (IQR), Friedman Test Statistic And |Z| Value Across Treatment Timelines for Mastication Note: I – Pre-treatment; II – Post-treatment; III – Follow-up after 1 month. *Significant at 0.05 level of significance with adjusted alpha (p<0.017). Table 1: Median, Inter Quartile Range (IQR), Friedman Test Statistic And |Z| Value Across Treatment Timelines for Mastication Observation Evaluation.
The non-parametric Friedman’s Test was also used to compare sEMG parameters such as amplitude, chew duration, and inter-chew duration across pre-, post- treatment and follow-up conditions. It can be noted from the median values that there was an increase in amplitude across sessions, whereas both the duration parameters decreased across sessions. The findings thus indicate that there was an improvement in all the three sEMG parameters. Further, pairwise comparisons using Wilcoxon Signed Rank test revealed that there was a significant difference in all the 3 sEMG parameters in both the left and right masseter muscles in the pre- versus post-therapy and pre- versus follow-up conditions at 0.05 level of significance. The results have been depicted in Table 2 below.
| sEMG parameters | Median (IQR) | Friedman’s test statistic X²(2) | Pairwise comparisons |Z| | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Amplitude (µV) | Rt | I | |||||||||
| Lt | |||||||||||
| Chew Duration (ms) | Rt | ||||||||||
| Lt | |||||||||||
| Inter Chew Duration (ms) | Rt | ||||||||||
| Lt | |||||||||||
| Amplitude (µV) | Rt | II | 37.5 (26.2) | 10.33 | 2.20* | 1.78 | 2.20* | ||||
| Amplitude (µV) | Rt | III | 43.7 (12.6) | 10.33 | 2.20* | 1.78 | 2.20* | ||||
| Amplitude (µV) | Lt | II | 33.2 (12.0) | 12 | 2.20* | 1.78 | 2.20* | ||||
| Amplitude (µV) | Lt | III | 40.8 (10.3) | 12 | 2.20* | 1.78 | 2.20* | ||||
| II | Chew Duration (ms) | Rt | 617.4 (303.7) | ||||||||
| III | Chew Duration (ms) | Rt | 474.6 (135.9) | ||||||||
| Lt | Chew Duration (ms) | II | 681.5 (384.0) | 10.33 | 10.33 | 2.20* | 1.57 | 2.20* | 2.20* | 1.79 | 2.20* |
| Lt | Chew Duration (ms) | III | 515.3 (218.4) | 10.33 | |||||||
| Inter Chew Duration (ms) | Rt | II | 624.8 (455.6) | 9.33 | 2.20* | 1.57 | 2.20* | ||||
| Inter Chew Duration (ms) | Rt | III | 344.9 (92.5) | 9.33 | 2.20* | 1.57 | 2.20* | ||||
| Inter Chew Duration (ms) | Lt | II | 759.5 (485.4) | 9.3 | 2.20* | 1.57 | 2.20* | ||||
| Inter Chew Duration (ms) | Lt | III | 359.6 (178.8) | 9.3 | 2.20* | 1.57 | 2.20* | ||||
Table 2: Median, Inter Quartile Range (IQR), Friedman Test Statistic and |Z| Value Across Treatment Timelines for Semg **Note:**
Table 2: Median, Inter Quartile Range (IQR), Friedman Test Statistic and |Z| Value Across Treatment Timelines for Semg Note: I – Pre-treatment; II – Post-treatment; III – Follow-up after 1 month. Rt – Right masseter; Lt – Left masseter. *Significant at 0.05 level of significance with adjusted alpha (p<0.017). Table 2: Median, Inter Quartile Range (IQR), Friedman Test Statistic and |Z| Value Across Treatment Timelines for Semg Parameters.
Discussion
The findings of the study highlight the improvement in masticatory dynamics as evinced by the scores of both the subjective and objective assessment tools. There was a significant change in the different masticatory outcome measures after the intensive FCT program. This is in agreement with the findings of recent studies which have reported that FCT is effective in improving the chewing abilities in addition to reducing tongue thrust and drooling in children with CP [7, 20]. However, these studies employed a parent-delivered program and also compared the overall chewing performance and feeding behaviors by using only subjective tools.
The MOE is a reliable and valid tool that assesses the isolated oromotor movements involved in chewing. The results indicated enhanced functioning of the oral structures in chewing. There was an improvement in jaw, lip, tongue and overall masticatory coordination contributing to better masticatory performance. FCT facilitated better lip seal, jaw stability and tongue lateralization in the post-therapy and follow-up conditions, aiding in effective chewing and swallowing. As a result, all the participants were able to successfully transition from pureed or mashed consistencies to safely ingest easy-to-chew solid food.
The present study is one of the first to use an objective tool such as sEMG to assess masticatory efficiency across a chewing training program. Studies have shown that the weakness in the masticatory muscles in children with CP leads to increased muscle contraction duration and reduced amplitude [21, 22, 23, 24]. The sEMG results indicated an increase in jaw strength and masticatory control, exemplified by the changes both in terms of amplitude and duration measures of the right and left masseter muscles. The significant difference observed in the pre- versus post-therapy and follow-up conditions indicates an optimistic outcome with respect to the duration of therapy and the components involved in the intervention. The fact that 20 sessions of training could notably improve muscle strength and functioning is encouraging for SLPs, since a concise therapy plan for feeding is the need of the hour as there is a shortage of pediatric feeding therapists, whereas the demand for dysphagia therapy is huge.
It is interesting to note that both in MOE and sEMG, there was an improvement in pre- versus post-therapy and pre- versus follow-up conditions. This could indicate that the functional changes in oral structures occur in close association with neuromuscular changes across the 20 sessions of chewing training. The continued improvement after therapy shows that though the chewing exercises are not being performed overtly, better management and progression of food textures leads to inclusion of variety in the diet, which reflects improved muscle strength and masticatory performance and no detraining effect. The significant difference in the pre-post condition for both objective and subjective measures could indicate that the duration of the training program is sufficient to stabilize muscle strength and functioning.
No significant difference in all the MOE and sEMG parameters, except overall MOE scores between the post- therapy versus follow-up conditions, indicate that the improvements though present were small, suggesting a lack of detraining effect. However, these minor improvements cannot be considered insignificant as they signify the neurodevelopmental and oromotor changes which are occurring as a result of inclusion of various textures in the diet of the participants. As indicated previously, the cessation of chewing exercises and orosensory stimulation could have led to a deceleration in the oromotor movements associated with mastication. Interestingly, a significant change was seen across all the three timelines in the overall mastication scores on MOE, which is encouraging. The individual jaw, lip and tongue scores when added up showed a significant change, which could indicate the interactive relationship between parameters. Therefore, conducting the study on a larger population might provide more conclusive evidence regarding treatment effects and this will help in generalizing the results better.
Conclusions
The present study is a preliminary attempt in the Indian context and adds to the small body of research on mastication in pediatric feeding disorders, particularly those with cerebral palsy. The findings provide noteworthy evidence to elucidate the efficacy of the FCT program by illustrating the changes in jaw, lip, tongue abilities during chewing and in amplitude and durational parameters contributing to better masticatory performance. The present study is one of the first to use objective assessments such as sEMG to assess masticatory efficiency across a chewing training program. The limitation of the study is the small sample size.
Future studies need to include multiple functional outcome measures to document the impact of chewing training on the quality of life using a larger sample.
Acknowledgements: We would like to thank the University of Mysore for the support rendered. We also wish to thank the Director, AIISH, Mysuru for providing the infrastructure for the study. Lastly, we express our gratitude to all the participants and the parents. Contributors: KV and SN – conceived and designed the study; KV: collected the data; KV: analysis and interpretation of data; KV and SN: drafting the manuscript; Both the authors approved the final manuscript. Funding Agency: None. Conflicts of Interest: There are no conflicts of interest.
References
-
Foster KD, Woda A, Peyron MA (2006) Effect of texture of plastic and elastic model foods on the parameters of mastication. J Neurophysiol 95(6): 3469-3479.
-
Chen J (2009) Food oral processing - A review. Food Hydrocoll 23(1): 1-25.
-
American Speech-Language-Hearing Association. (n.d). Pediatric Feeding and Swallowing. https://www.asha. org. 14 December, 2022.
-
Le Reverend BJ, Edelson LR, Loret C (2014) Anatomical, functional, physiological and behavioral aspects of the development of mastication in early childhood. Br J Nutr 111(3): 403-414.
-
Nicklaus S, Demonteil L, Tournier C (2015) Modifying the texture of foods for infants and young children. Modifying Food Texture pp: 187-222.
-
Cichero JA, Murdoch BE (2006) Dysphagia: Foundation, theory and practice. John Wiley & Sons New York, USA, pp: 1-572.
-
Inal O, Arslan SS, Demir N, Yilmaz OT, Karaduman AA (2017) Effect of functional chewing training on tongue thrust and drooling in children with cerebral palsy: A randomised controlled trial. J Oral Rehabil 44(11): 843- 849.
-
Poinsett PM (2020) Cerebral palsy facts and statistics. Cerebral palsy guidance.
-
Shahanawaz SD, Palekar TJ, Shah N (2015) Effect of Swiss ball on balance in children with spastic diplegia: A case study. International Journal of Research in Pediatrics Journal of Pediatrics 1(1): 8-11.
-
Lopes PAC, Amancio OMS, Araujo RFC, Vitalle MSDS, Braga JAP (2013) Food pattern and nutritional status of children with cerebral palsy. Rev Paul Pediatr 31(3): 344-349.
-
Arslan SS, Demir N, Inal O, Karaduman AA (2018) The severity of chewing disorders is related to gross motor function and trunk control in children with cerebral palsy. Somatosens Mot Res 35(3-4): 178-182.
-
Gangil A, Patwari AK, Aneja S, Ahuja B, Anand VK (2001) Feeding problems in children with cerebral palsy. Indian Pediatr 38(8): 839-846.
-
Prathima S, Kumar P, Swapna N, Shabnam S (2015) Feeding and oromotor problems in children with cerebral palsy: A survey. J All India Inst Speech Hear 34: 36-47.
-
Eckman N, Williams KE, Riegel K, Paul C (2008) Teaching chewing: A structured approach. Am J Occup Ther 62(5): 514-521.
-
Gibbons BG, Williams KE, Riegel KE (2007) Reducing tube feeds and tongue thrust: Combining an oral–motor and behavioral approach to feeding. Am J Occup Ther 61(4): 384-391.
-
Baghbadorani MK, Soleymani Z, Dadgar H, Salehi M (2014) The effect of oral sensorimotor stimulations on feeding performance in children with spastic cerebral palsy. Acta Med Iran 52(12): 899-904.
-
Gisel EG, Applegate-Ferrante T, Benson J, Bosma JF (1995) Effect of oral sensorimotor treatment on measures of growth, eating efficiency and aspiration in the dysphagic child with cerebral palsy. Dev Med Child Neurol 37(6): 528-543.
-
Gisel EG, Applegate-Ferrante T, Benson J, Bosma JF (1996) Oral-motor skills following sensorimotor therapy in two groups of moderately dysphagic children with cerebral palsy: Aspiration vs nonaspiration. Dysphagia 11(1): 59-71.
-
Sigan SN, Uzunhan TA, Aydinli N, Eraslan E, Ekici B, et al. (2013) Effects of oral motor therapy in children with cerebral palsy. Ann Indian Acad Neurol 16(3): 342-346.
-
Arslan SS, Demir N, Karaduman AA (2017) Effect of a new treatment protocol called Functional Chewing Training on chewing function in children with cerebral palsy: A double‐blind randomized controlled trial. J Oral Rehabil 44(1): 43-50.
-
Arslan SS, Demir N, Dolgun AB, Karaduman AA (2016) Development of a new instrument for determining the level of chewing function in children. J Oral Rehabil 43(7): 488-495.
-
Remijn L, Speyer R, Groen BE, Van Limbeek J, Nijhuis- van der Sanden MW (2014) Validity and reliability of the Mastication Observation and Evaluation (MOE) instrument. Res Dev Disabil 35(7): 1551-1561.
-
Briesemeister M, Schmidt KC, Ries LGK (2013) Changes in masticatory muscle activity in children with cerebral palsy. J Electromyogr Kinesiol 23(1): 260-266.
-
Giannasi LC, Matsui MY, Politti F, Batista SRF, Caldas BF, et al. (2014) Test–retest reliability of electromyographic variables of masseter and temporal muscles in patients with cerebral palsy. Arch Oral Biol 59(12): 1352-1358.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?