A Huge Solitary Peripheral Osteoma of Mandible: A Case Report
Osteoma is a benign, slow-growing tumor composed of mature compact or cancellous bone. They originate from the craniomaxillo facial region such as temporal bones, sinuses, maxilla or mandible. Patients with osteomas should be evaluated for Gardner’s syndrome (GS). The treatment for osteoma is surgical excision if the lesion is symptomatic. We present a case of a solitary peripheral osteoma (PO) arising from the superior aspect of ramus of mandible causing facial asymmetry in a 22-yearold man.
Introduction
Osteomas are benign, slow-growing lesion composed of compact or cancellous bone. They mostly occur between 2nd and 5th decades, but may be seen at any age. They can occur as solitary or multiple lesions. Solitary osteomas may be classified as: peripheral, arising from the periosteum, central, arising from the endosteum and extra skeletal, arising in soft tissue [1]. Multiple osteomas may be associated with Gardner’s syndrome.
Case Report
A 22-year-old man presented to Otorhinolaryngology- head and neck surgery department of tertiary health care center with complaints of swelling of left cheek for 1 year. Swelling was of gradual onset and slowly increased in size to attain the present size. It was associated with pain and asymmetry of face.


There was no history of difficulty opening of mouth, chewing, swallowing and breathing. He had no previous facial trauma or significant medical history. On inspection a hard, tender, non-pulsatile swelling noted on left malar region with facial asymmetry. The overlying skin was normal in color and showed no adhesion to the mass (Figure 1). Intraorally a smooth, tender, hard swelling was present in oropharynx region pushing the left tonsil and tonsillar pillars to midline (Figure 2).

Plain Computed Tomography (CT) scan was done which showed a large well defined multilobulated bone density lesion measuring approximately 66 x 50 x 42 mm in left infratemporal fossa. Medially the lesion was extending and involving left parapharyngeal space with displacement of left lateral wall of nasopharynx towards contralateral side, it was involving pterygoid muscle with scalloping of left lateral pterygoid plate, posteriorly the lesion was abutting left styloid process , anteriorly the lesion was abutting and scalloping posterior wall of left maxillary sinus and laterally the lesion was abutting condyle and coronoid process of mandible along with scalloping of the superior ramus of mandible suggestive of osteoma of superior aspect of left ramus of mandible (Figure 3).
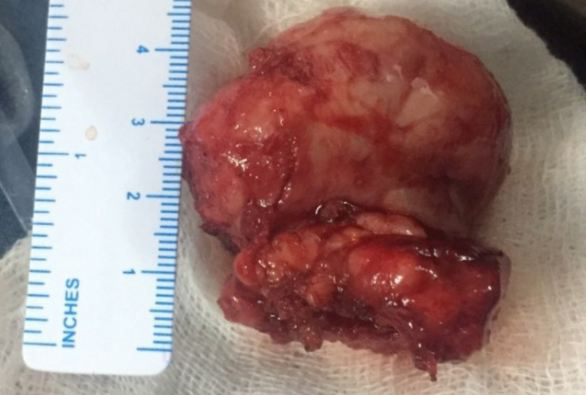
Patient has no symptoms suggestive of GS. Blood investigations were within normal limits. Patient underwent surgical intervention under general anesthesia and mass was removed with preauricular infratemporal approach. Histopathological examination of surgical specimen (Figure 4) was done and result came out as osteoma. Patient was followed up every 6months and there was no recurrence till now.
Discussion
Osteoma can occur at any age but most commonly diagnosed between third and fifth decades and are more common in males than in females [2]. The exact etiology and pathogenesis of osteoma is unknown. Some authors consider them as true neoplasms, while others classify them as developmental anomalies [1].
In maxillofacial area, osteoma occurs most frequently in the sinuses. The most common site is frontal sinus, followed by maxillary and ethmoidal sinuses [3]. It has also been described in external auditory canal, temporal bones, maxilla and mandible. Peripheral osteoma of jaw bones is quite rare. An osteoma may be clinically silent for years and usually diagnosed when it becomes enlarged causing facial asymmetry (as in our case) and functional impairment or is incidentally discovered by radiological examination.
GS should be suspected in patients with facial osteoma. This syndrome is an autosomal dominant disease characterized by gastrointestinal polyps, multiple osteomas, skin and soft tissue tumors, and multiple impacted or supernumerary teeth. Intestinal polyps are mostly adenomas and may progress to malignancy in almost 100% of patients [1].
The treatment for osteoma is surgical excision, if there is painful or active lesion growth, facial asymmetry or other secondary problems, such as blockage of cavities, nerve foramina, and vital organ compression. Removal of an asymptomatic osteoma is not necessary. Surgery consists of removing the lesion at the base where it enters the cortical bone. Malignant transformation has not been reported in the literature [4]. Though recurrence is not commonly reported, routine clinical and radiographic follow up is advised.
Conclusion
Although osteoma of jaw region is rare, it may grow large and cause cosmetic disfigurement and functional impairment. In patients with osteoma of the facial skeleton, possibility of GS should be kept in mind. Osteomas often develop before the colorectal polyposis and early diagnosis of syndrome may be lifesaving in certain cases. Though recurrence of osteoma after surgical excision is extremely rare, routine follow-up is recommended.
Author Contributions
Sonika Dhari Shrestha: drafting and compiling of article, getting consent from patient;
Tridip Pantha: supervision and correction of drafted article;
Dipendra Gautam: supervision and correction of drafted article
Disclosures
Competing interests: None. Sponsorships: None. Funding source: None. Ethical clearance: Approval from IRB is not required for case report in our institute
References
-
Sayan NB, Uçok C, Karasu HA, Günhan O (2002) Peripheral osteoma of the oral and maxillofacial region: a study of 35 new cases. J Oral Maxillofac Surg 60(11): 1299-1301.
-
Wanyura H, Kamiński A, Stopa Z (2005) Treatment of osteomas located between the anterior cranial base and the face. J Craniomaxillofac Surg 33(4): 267-275.
-
Larrea-Oyarbide N, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C (2008) Osteomas of the craniofacial region. Review of 106 cases. J Oral Pathol Med 37(1): 38- 42.
-
Woldenberg Y, Nash M, Bodner L (2005) Peripheral osteoma of the maxillofacial region. Diagnosis and management : A study of 14 cases. Med Oral Patol Oral Cir Bucal 10(S2): E139-E142.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?