Nasal and Skull Base Reconstruction with Turbinate Flaps
Introduction: The reconstruction of the skull base and nasal mucosa can be performed using different local flaps. The use of the nasoseptal flap is the most common method to reconstruct these areas, but sometimes, due to septal perforations, a history of previous surgeries that may have damaged its pedicle, or because its rotational arc is not ideal, other nasal flaps such as those from the inferior or middle turbinate with their various pedicles may need to be employed. Objectives: The aim of this study was to ascertain the success rate of reconstructions involving the nasal cavity and skull base utilizing inferior and middle turbinate flaps. Methods: Data collected prospectively were analyzed using an Excel spreadsheet for patients who underwent skull base and nasal cavity defect repairs employing turbinate flaps between May 2014 and August 2021. Results: Nine patients were treated and a total of ten reconstructions were performed. Five middle turbinate flaps were executed, two involving medial rotation to address defects situated on the ethmoid roof and three involving lateral rotation to repair a defect within the ethmoid fovea, with two of these flaps closing the frontal ostium. Furthermore, an inferior turbinate flap with a posterior pedicle was utilized to repair the defect resulting from the resection of a meningocele, which was located on the ethmoid roof. Four lateral wall flaps with an anterior pedicle were employed to reconstruct the mucosa of the nasal cavity and to address a defect in the anterior skull base. Conclusion: The reconstruction of anterior skull base defects using turbinate flaps was highly satisfactory, achieving a 100% success rate. The use of lateral wall flaps to repair defects produced by rhinectomies that included resection of the nasal mucosa was also successful and we did not have partial or total necrosis of the flaps. The excellent blood supply to the lateral nasal walls and the ability to dissect these flaps with different arterial pedicles and extend their surface, including the nasal floor, allows for various flap rotations and the reconstruction of defects of different sizes.
Introduction
Reconstruction of the skull base can be achieved through various techniques. The use of grafts can be beneficial for small defects, employing a multi-layer repair technique. Nasal flap reconstruction is preferred when the defect exceeds 1cm in size, when there is a high-flow cerebrospinal fluid leak, or when the patient has undergone or will undergo radiotherapy. Nasal flaps can also be utilized for reconstructing the mucosal lining of the nasal cavity. These flaps are within the same surgical field and can be dissected using the same endonasal approach employed to address the pathology. The most commonly used flap is the nasoseptal flap, but in cases where this cannot be utilized, inferior and middle turbinate flaps can serve as an excellent option for reconstruction due to their robust vascularization and versatility in rotation, as they can be dissected with various pedicles.
Objectives
To determine the success rate of nasal cavity and skull base reconstructions using inferior and middle turbinate flaps.
Methods
Prospective data analysis was conducted using an Excel spreadsheet for patients in whom inferior and middle turbinate flaps were employed for repairing defects in the skull base and nasal cavity between May 2014 and August 2021. Patients who had received nasoseptal flaps or grafts for repair were excluded from the study.
The collected data included the patients age and gender, presenting signs or symptoms, site of repair, type of turbinate flap used, flap pedicle, complications, and the success or failure of the reconstruction.
The turbinate flaps used included: lateral or medial rotation of the middle turbinate, posterior pedicle of the inferior turbinate, and anterior or posterior pedicle of the lateral wall turbinate.
All surgeries were performed under general anesthesia via an endonasal approach with 0° endoscopes, and a cautery with straight and curved Colorado-tip was used. After locating the defect, the surrounding mucosa was resected, and the bone was exposed.
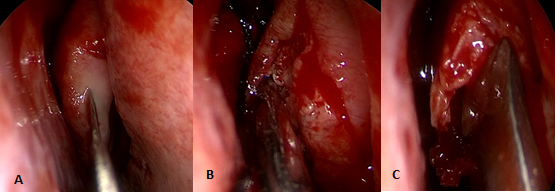
In cases of middle turbinate flaps, the anterior aspect was incised with a scalpel or cautery, and the mucoperiosteum of the medial and lateral aspects of the turbinate was dissected, with the underlying turbinate bone being resected see Figure 1.
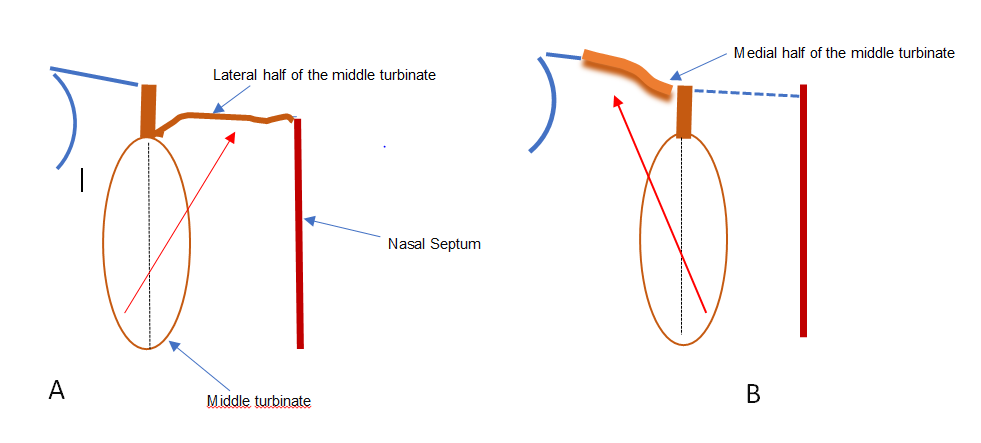
If the flap was used to repair the area of the skull base between the nasal septum and the middle turbinate, the medial half of the middle turbinate was resected, and the lateral half was rotated to cover the defect.
In some patients, intradural fat was placed in the defect before applying the mucoperiosteal flap. If the lateral area of the skull base was repaired (between the middle turbinate and the lamina papyracea of the ethmoid bone), the lateral half of the middle turbinate was resected, and the medial half was rotated laterally see Figure 2.
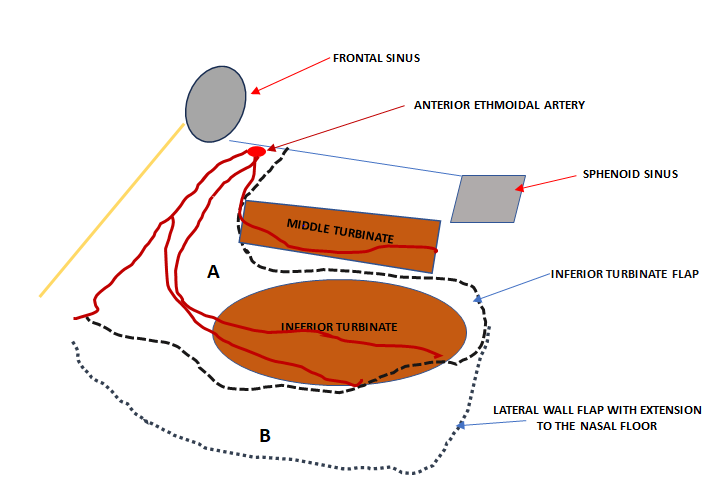
In the case of inferior turbinate flaps with a posterior pedicle, an incision was made with cautery in front of the turbinate head, and the mucoperiosteum of the turbinate bone was dissected and removed. The anterior incision was extended above and below the turbinate, taking care not to damage the posterior lateral nasal artery or the sphenopalatine artery. When the flap with an anterior pedicle was used, the posterior, superior, and inferior incisions were made first, from back to front, with cauterization of the sphenopalatine or posterior lateral nasal artery, leaving a broad base of anterior-superior implantation. In the lateral wall flap reconstructions, the technique was similar, but the floor of the nasal cavity was included to obtain a larger flap surface see Figure 3.
In skull base reconstructions, after the flap repair, Surgiflo was applied, followed by anterior packing using a Merocel placed inside a finger of a glove, which was removed after 4 days.
Antibiotics were prescribed for 10 days. Patients were kept in the intermediate care unit for 4 days. Rest and all necessary measures to reduce intracranial pressure were advised. The reconstruction was considered successful when the patient no longer experienced cerebrospinal fluid leakage, when nasal mucosal reconstruction was effective, or when the patient’s symptoms were successfully resolved.
Results
A total of 9 patients were treated, including 5 men and 4 women. The youngest patient was 27 years old, and the oldest was 94. The average age was 63.1 years. There were 10 reconstructions performed.
The treated pathologies that required reconstruction with inferior and middle turbinate flaps included: meningoceles located in the ethmoidal cribriform plate (3/9), cranial trauma with pneumocephalus (1/9), defects at the level of the floor of the frontal sinus and post-chemotherapy/ radiotherapy cribriform plate, and cranio-endoscopic resection of the frontal sinus and ethmoid for carcinomas (2/9), pneumocephalus following neurosurgical resection of a meningioma where the floor of the frontal sinus was obliterated (1/9), and three mucosal reconstructions of the nasal cavity after a rhinectomy.
Five middle turbinate flaps were created, two with medial rotation to repair defects located on the roof of the ethmoid, between the middle turbinate and the nasal septum (Figure 4), and three with lateral rotation to repair a defect in the ethmoid fovea and two to obliterate the frontal ostium Figure 5&6.
In the three patients with meningoceles, after exposing the bony edges of the defect and reducing the lesion with bipolar cautery, intradural fat was placed, followed by the turbinate mucoperiosteal flap.
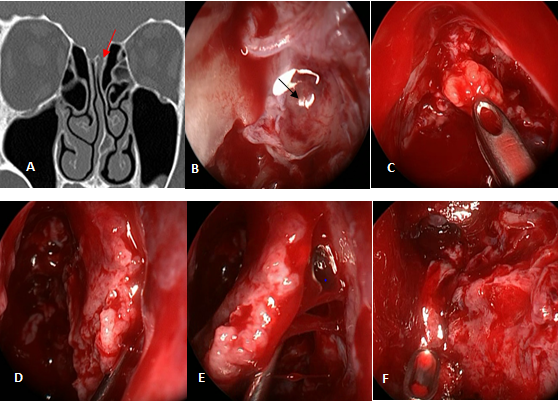
Figure 4: Ethmoid Meningocele A: Computed Tomography (Arrow Indicates the Meningocele); B: Meningocele (Arrow); C: Intradural Fat Placement After Reducing the Meningocele with Bipolar Cautery; D: Resection of the Medial Half and Bone of the Middle Turbinate; E: Medial Rotation of the Lateral Mucoperiosteum of the Middle Turbinate; E: Defect Repair.
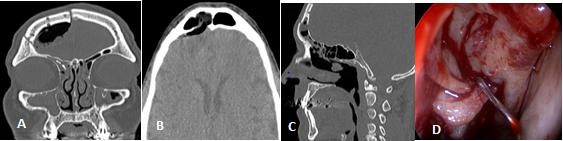
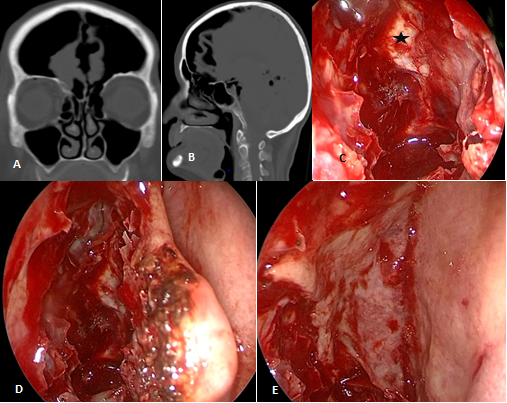
Figure 5: Postoperative Pneumocephalus Following a Craniotomy and Defective Frontal Sinus Obliteration. A, B, C: Computed Tomography Showing Discontinuity of the Posterior Wall of the Frontal Sinus and Neumocephalus; D: Draf II-A and Obliteration of the Frontal Sinus Ostium with a Bipedicle Middle Turbinate Mucoperiosteal Flap with Lateral Rotation.
A flap of the inferior turbinate with a posterior pedicle (posterior-lateral nasal branch of the sphenopalatine artery) was used to repair the defect left by the resection of a meningocele located on the ethmoidal roof between the middle turbinate and the septum.
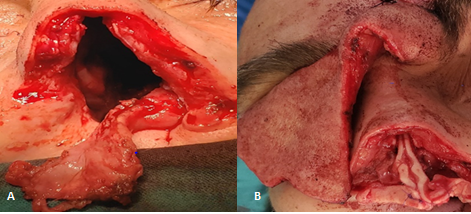
Four lateral wall flaps (inferior turbinate + mucoperiosteum of the nasal floor) with an anterior pedicle (ethmoidal arteries and a branch of the facial artery) were used to reconstruct nasal cavity mucosa and repair a defect in the anterior skull base (Figure 7).
There were no intraoperative or postoperative complications.
Reconstruction was considered successful when cerebrospinal fluid leakage, pneumocephalus, and nasal cavity mucosal lining were adequately resolved. Follow- up assessments of the repair were conducted using nasal endoscopy and computed tomography (Table 1).
| Sex | Age | Sign/symptom | Repair site | Flap | Pedicle | complications | Success |
|---|---|---|---|---|---|---|---|
| M | 27 | pneumoencephalus | cribriform plate meningocele | inferior turbinate | posterior | no | yes |
| F | 62 | cranioliquorrhea | cribriform plate meningocele | middle turbinate | medial | no | yes |
| F | 94 | pneumoencephalus | ethmoidal fovea trauma | middle turbinate | lateral | no | yes |
| F | 37 | cranioliquorrhea | cribriform plate meningocele | middle turbinate | medial | no | yes |
| F | 61 | undifferentiated carcinoma: QT+RT + cranionasal surgery | frontal sinus floor and right cribriform plate | lateral wall | anterior | no | yes |
| M | 75 | squamous cell carcinoma/ rhinectomy | nasal cavity mucosa | lateral wall | anterior | no | yes |
| M | 77 | squamous cell carcinoma/ rhinectomy due to recurrence in previous case, 2 years later | nasal cavity mucosa | lateral wall | anterior | no | yes |
| M | 61 | squamous cell carcinoma/ rhinectomy | nasal cavity mucosa | lateral wall | anterior | no | yes |
| M | 59 | pneumocephalus after meningioma resection | frontal sinus floor | middle turbinate | lateral | no | yes |
| M | 78 | squamous cell carcinoma: QT+RT and then cranionasal surgery | frontal sinus | middle turbinate | lateral | no | yes |
Table 1: Reconstructions Performed with Turbinate Flaps to Reconstruct the Skull Base and Nasal Cavity.
Discussion
The reconstruction of the skull base has evolved since the description of the nasoseptal flap by Drs. Hadad-Basagastegui in 20061. Most defects in the skull base measuring less than 1 cm can be satisfactorily repaired (>90% success rate) with grafts or flaps, preferably using a multilayer technique. Success in these cases is independent of the method and material used for reconstruction. The incidence of postoperative cerebrospinal fluid leaks for larger defects has decreased from 20-30% to less than 5% in anterior skull base reconstructions performed with vascularized flaps [1].
Flaps, due to their superior vascularity, are preferred for repairing defects larger than 1 cm, high-flow cerebrospinal fluid leaks, or when patients have undergone or will undergo chemotherapy and/or radiation therapy.
The nasoseptal flap is not advisable when patients have a history of septal surgery, surgical treatment or embolization of epistaxis, or perforations of the nasal septum. When the defect is located in the anterior skull base, the nasoseptal flap may not be the best reconstruction option because it may not reach the defect when pediculated posteriorly and rotated. In such cases, turbinate flaps, specifically inferior turbinate flaps, can be an excellent alternative.
Inferior turbinate flaps offer versatility in reconstruction, as they can be rotated with either a posterior pedicle (posterior lateral nasal artery) or an anterior pedicle (anterior ethmoidal artery, lateral nasal artery, and angular artery, which are branches of the facial artery) [2, 3]. In addition, the mucoperiosteum of the nasal floor can be included to repair larger defects (lateral wall flap).
In our study, we successfully used a posterior-pedicled inferior turbinate flap to repair a defect following the resection of a meningocele located in the ethmoidal roof between the middle turbinate and the septum. Four lateral wall nasal flaps with anterior pedicles (ethmoidal arteries and a branch of the facial artery) were used to reconstruct the nasal mucosa and repair a defect in the anterior skull base. There were no intraoperative or postoperative complications.
There are limited reports in the literature on the use of turbinate flaps for mucosal reconstruction after rhinectomy. Langdon, et al. [4] conducted a study on 10 cadavers and reported that lateral wall flaps could be used to reconstruct defects measuring approximately 4 cm by 2.5 cm, and extending the flap to the nasal floor allowed for repairs of 5 cm by 5 cm defects. They also described a clinical case in which this flap was used for reconstruction after rhinectomy without skin resection.
The mucoperiosteal middle turbinate flap was described by Prevedello, et al. [5] in 2009. This flap can be used to repair defects in the sellar region, ethmoidal fovea, ethmoidal cribiform plate, and sphenoid plane. The average length and width of the flap can be 4.04 cm by 2.8 cm. It has a posterior pedicle, which is the middle turbinate’s vascular supply originating from the posterior lateral nasal artery of the sphenopalatine artery. Dissecting this flap posteriorly to the sphenopalatine foramen can increase its length. Other studies describe that the primary blood supply for the middle turbinate’s medial mucoperiosteum comes from the anterior, posterior, and sometimes the middle ethmoidal arteries, while the lateral sector is supplied by the middle turbinate artery, a branch of the posterior lateral nasal artery.
Both sectors have one or more anastomoses on the anteroinferior edge of the middle turbinate [6, 7].
By dissecting the medial or lateral mucoperiosteum and rotating the flap like a hinge, both pedicles can be preserved, ensuring the flap’s vitality even if one pedicle is damaged. Most studies use a posterior-pedicled middle turbinate flap [8, 9].
Perhaps this is the best technique for the flap to reach the sellar region.
In reconstructions of the ethmoid fovea or cribriform plate, the medial or lateral rotation of the flap allows for repairing the skull base while preserving the two pedicles. Only Schreiber’s study6 describes this bipedicle flap modality used to repair a defect in the ethmoid roof.
In our study, we used the bipedicle middle turbinate flap in five skull base defects. In two cases of meningoceles located in the cribriform plate of the ethmoid, a multilayer reconstruction was performed, including intradural fat placement followed by the bipedicle mucoperiosteal flap of the middle turbinate, with the lateral half rotated medially to repair the defect.
In another larger defect that resulted in a pneumocephalus, located lateral to the middle turbinate in the ethmoid fovea, only a bipedicle flap was used, with the medial half of the turbinate rotated laterally to repair the defect using an “over” technique.
In another patient without cerebrospinal fluid leakage, with progressive tension pneumocephalus following a craniotomy for meningioma resection, the bipedicle middle turbinate flap with lateral rotation was used to obliterate the frontal recess and resolve the pneumocephalus. In the third case, the same technique was used to reinforce closure in an endonasal cranial approach performed for persistent squamous cell carcinoma of the frontal sinus following chemoradiotherapy.
The advantages of this flap are that it can be used when the sphenopalatine artery is damaged (irrigation from ethmoidal arteries) and that it is located in the same surgical field as the defect to be repaired.
The disadvantages include that flap dissection may be more challenging if the bony attachment of the middle turbinate is destabilized. Anatomic variations (25%) [10] that may complicate dissection, such as a bullous, paradoxical, or hypoplastic turbinate, can also exist.
In many endonasal approaches to the skull base, middle turbinate turbinectomy is a step in the surgical technique. We believe that routine resection of the middle turbinate should be avoided to preserve an important method for skull base reconstruction.
In a study Shibu GM, et al. [11], a 100% success rate was reported in skull base reconstruction using a posterior- pedicled middle turbinate flap. Twenty patients had cerebrospinal fluid leaks localized in the ethmoidal cribiform plate, lateral to the middle turbinate lamella (11/20), medial to the lamella (3/20), and in the sellar region (6/20).
Simal, et al. [12] reported successful skull base reconstruction in 10 patients with a middle turbinate flap with posterior pedicle after endoscopic approaches to the sellar and suprasellar regions.
Conclusion
The reconstruction of anterior skull base defects using turbinate flaps was highly satisfactory, achieving a 100% success rate.
The use of lateral wall flaps to repair defects produced by rhinectomies that included resection of the nasal mucosa was also successful and we did not have partial or total necrosis of the flaps.
The excellent blood supply to the lateral nasal walls and the ability to dissect these flaps with different arterial pedicles and extend their surface, including the nasal floor, allows for various flap rotations and the reconstruction of defects of different sizes.
Conflict of Interest Statement
“The authors declare no conflicts of interest related to this research.
References
-
Hadad G, Basagasteguy L, Carrau RL, Mataza JC, Kassam A, et al. (2006) A Novel Reconstructive Technique after Endoscopic Expanded Endonasal Approaches: vascular pedicle nasoseptal flap. Laryngoscope 116(10): 1882- 1886.
-
Hadad G, Rivera-Serrano CM, Bassagaisteguy LH, Carrau RL, Miranda JF, et al. (2011) Anterior Pedicle Lateral Nasal Wall Flap: A Novel Technique for the Reconstruction of Anterior Skull Base Defects. Laryngoscope 121(8): 1606-1610.
-
Al Shouk AAAHM, Tatar I (2021) The blood supply of the inferior nasal concha (turbinate): a cadaveric anatomical study. Anat Sci Int 96(1): 13-19.
-
Langdon C, Ato KY, Perez CP, Arancibia C, Alobid I (2021) Anterior Pedicled Lateral Nasal Wall Flap for Endonasal Lining: A Radiologic and Anatomical Study. Laryngoscope 131(5): E1462-E1467.
-
Prevedello DM, Coll JB, Fernandez Miranda JC, Morera V, Jacobson D, et al. (2009) Middle Turbinate Flap for Skull Base Reconstruction: Cadaveric Feasibility Study. Laryngoscope 119(11): 2094-2098.
-
Schreiber A, Mattavelli D, Ferrari M, Rampinelli V, Lancini D, et al. (2017) The turbinal flap: an additional option for anterior skull base reconstruction. Cadaveric feasibility study and case report. International Forum of Allergy & Rhinology 7(2): 199-204.
-
MacArthur FJD, McGarry GW (2016) The arterial supply of the nasal cavity. European Archives of Oto-Rhino- Laryngology 274: 809-815.
-
Wang X, Zhang X, Hu F, Yu Y, Gu Y, et al. (2016) Middle Turbinate Mucosal Flap in Endoscopic Skull Base Reconstruction. Turk Neurosurg 26(2): 200-204.
-
Tamura R, Toda M, Kohno M, Watanabe Y, Ozawa H, et al. (2016) Vascularized middle turbinate flap for the endoscopic endonasal reconstruction of the anterior olfactory groove. Neurosurg Rev 39(2): 297-302.
-
Perez-Pinas I, Sabate J, Carmona A, Catalina-Herrera CJ, Castellanos JJ (2000) Anatomical variations in the human paranasal sinus region studied by CT. Journal of Anatomy 197(2): 221-227.
-
Shibu G, Sandeep S (2017) Vascularized middle turbinate mucoperiosteal flap in skull base defects: follow-up analysis of 20 cases. International Journal of Otorhinolaryngology and Head and Neck Surgery 3(1): 71-76.
-
Simal Julian JA, Lloret PM, Ruiz-Valdepeñas EC, Coll JB, Giner AB, et al. (2011) Middle turbinate vascularized flap for skull base reconstruction after an expanded endonasal approach. Acta Neurochir 153(9): 1827-1832.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?