Clinicals and Audiometrics Aspects of Presbycusis in Senegal
Introduction: Presbycusis is a hearing impairment linked to the normal, natural and psycho-sensory ageing of the auditory organ as a whole. Several epidemiological studies have been carried out on this subject in developed countries. In Frenchspeaking Africa, presbycusis has received very little attention in the ENT literature. The aims of this study were to estimate the frequency of presbycusis and to describe the sociodemographic, clinical and audiometric factors involved. Patients and Methods: This is a descriptive, cross-sectional study carried out in the ENT Department of the Fann Hospital, during a humanitarian mission to distribute hearing aids. The study included all cases of presbycusis. The inclusion criteria were patients aged 50 and over with a deafness of bilateral and symmetrical perception on tonal audiometry. Sociodemographic, clinical, audiometric and therapeutic data were recorded. The data was analysed using SPSS (Statistical Package for Social Sciences) version 20. Results: Presbycusis represented 14.2% of patients who consulted for hearing loss. The sex ratio was 1.3 and the mean age was 68.88, with extremes of 50 and 95 and a standard deviation of 9.57. The consultation time was 9.19 years. Patients with moderate hearing loss accounted for 51.6%. Of the presbycusis patients, 82.03% were fitted with hearing aids. Conclusion: Presbycusis will increase at the same time as the life expectancy of our populations. Its treatment relies on hearing aids, which are expensive, hence the need for public authorities to get involved.
Introduction
Presbycusis is a hearing impairment linked to the normal, natural and psycho-sensory ageing of the auditory organ as a whole. It’s a biological phenomenon that no one can escape; it starts between the ages of 20 and 30 and becomes socially embarrassing around the age of 40 or 50 [1].
As quality of life improves and life expectancy increases, presbycusis is playing an increasingly important role in the daily practice of African ENT doctors.
However, in Senegal, as in other developing countries, presbycusis is difficult to diagnose and, above all, difficult to treat. Hearing aids are still out of reach for the majority of our population. Added to this is the lack of motivation on the part of the patient and sometimes those around them, who are unable to find a solution to their illness.
Many epidemiological studies have been done on the subject in developed countries [2, 3]. In French-speaking Africa, presbycusis has received very little attention in the ENT literature.
All these are reasons that motivated our work on presbycusis.
The aims of this study were to estimate the frequency of presbycusis and to describe the sociodemographic, clinical and audiometric factors involved.
Patients and Methods
This is a cross-sectional, descriptive study, which took place in the ENT department of the National University Hospital of Fann, during a humanitarian mission to distribute hearing aids, from 27 to 30 November 2017. During this period, we identified all cases of presbycusis among patients suffering from hearing loss.
The inclusion criteria were patients aged 50 and over with bilateral and symmetrical sensorineural hearing loss as measured by pure tone audiometry. The patients are referred from all regions of Senegal by ENT doctors.
The following patients were excluded from the study
- Those with asymmetric hearing loss or cophosis
- Patients with a history of temporal bone trauma, ear surgery, chronic otitis with abnormal otoscopy, malaria or meningitis We called the patients to ask them to complete their files and carry out a post-fitting satisfaction survey. We did not perform speech audiometry on our patients.
Sociodemographic, clinical, audiometric and therapeutic data were recorded.
All the data was collected on a pre-established form. They were entered using Excel software. The data was analysed using SPSS (Statistical Package for Social Sciences) version 20. The descriptive study was carried out by calculating absolute and relative frequencies for the qualitative variables and averages and standard deviations for the quantitative variables.
The hearing loss threshold was calculated according to the recommendations of the International Bureau for Audiophonology (BIAP) [4]. The average hearing loss is equal to the average of the hearing losses in the frequencies 500, 1000, 2000 and 4000 Hz for one ear according to the BIAP.
At the end of this calculation, hearing loss was classified according to BIAP as follows
Mild Hearing Loss
Average audiometric loss between 21 and 40 Db.
Moderate Hearing Loss
1st degree: average audiometric loss between 41 and 55 dB.
2nd degree: average audiometric loss between 56 and 70 dB.
Severe Hearing Loss
1st degree: average audiometric loss between 71 and 80 dB.
2nd degree: average audiometric loss between 81 and 90 dB.
Profound Hearing Loss
1st degree: average audiometric loss between 91 and 100 dB.
2nd degree: average audiometric loss between 101 and 110 dB.
3rd degree: average audiometric loss between 111 and 119 dB.
Above 119 dB, the hearing loss is total; an average loss of 120 dB is referred to as cophosis.
This last value was not included in our study.
Results
In a population of 900 hearing impaired peope, we found 128 cases of presbycusis, a percentage of 14.2%.
Clinical Data
Gender: Our series consisted of 128 patients including 72 men (56%) and 56 women (44%) for a sex ratio of 1.3.
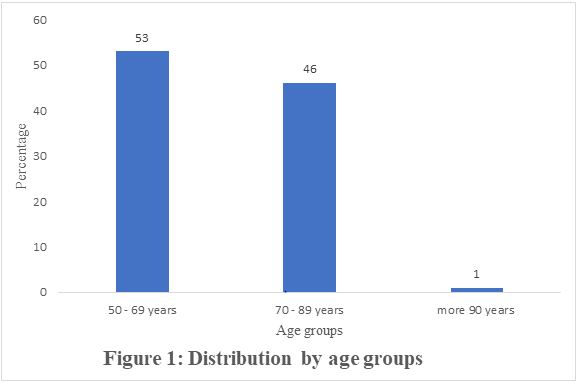
Age: The mean age in our series was 68.88 years, with extremes of 50 and 95 years and a standard deviation of 9.57. The ages were distributed as in Figure 1.
Consultation Time: The consultation time in our series was 9.19 years, with extremes ranging from one year to 30 years.
We have represented the time taken to consult a doctor by age group (Figure 2).
Analysis of the Clinical Factors of Presbycusis
Table 1 showed the distribution of patients according to the associated disease (diabetes, high blood pressure).
| Diabetes | n | % |
|---|---|---|
| Yes | 25 | 20 |
| No | 103 | 81 |
| High blood pressure | ||
| Yes | 63 | 49 |
| No | 65 | 51 |
Table 1: Presbyacousis, Diabetes and High Blood Pressure Distribution.
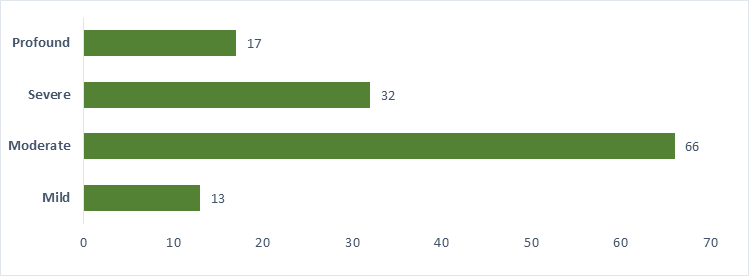
Associated Signs: Tinnitus was associated with presbycusis in 67% and dizziness in 43%. Audiometric Data: Tone audiometry was performed in all of our patients. We calculated the average hearing loss bilaterally according to BIAP (Figure 3).

Therapeutic Data: Of the presbycusis patients, 105 (82.03%) were fitted with hearing aids. Non-rehabilitated patients accounted for 17.97%. These were patients for whom the hearing aid offered no hearing benefit. Patients reported a clear improvement in hearing, even in noise, in 70.5% of cases.
Discussion
Clinical Aspects
Gender: The slight male predominance found in the series can be explained by the fact that auditory sensitivity decreases twice as quickly in men as in women at all frequencies and at all ages (Table II). Consequently, the age of onset of deafness is later in women at most frequencies and varies according to frequency [5]. In the same way Jerger and al report that presbycusis is more common in men than in women [6].
However, the exception noted in Brazil seems to be linked to the higher mortality rate among men and the difference in average age between spouses, with men being on average two years older than their partners [7].
Age: The average age of our patients was 68.88 years, it seems to have a relationship between age at diagnosis and life expectancy in Senegal, which was 66.9 years in 2018 [8]. Since presbycusis is an aging-related disease, the average age of patients is naturally variable depending on the populations studied. Thus it was 69.3 years in Nigeria [9]. Consultation Time: The consultation time was 9.19 years. This is a fairly long period of time which may be linked to the progressive nature of the deafness which is not initially bothersome for the patient. Guincharda AC reports that presbycusis is often unknown and that patients wait several years before consulting a hearing specialist [10].
Other prospective studies report a short delay of 2.6 years in Nigeria [11]. Associated Signs: Hearing loss is the main complaint in presbycusis, but it is often associated with tinnitus and dizziness. Sogebi OA in Nigeria in a series of 69 patients with presbycusis describes 79.7% tinnitus and 33.3% dizziness [11]. Our results are similar. A methodologically rigorous study carried out in Singapore concluded that vestibular disorders are not linked to presbycusis [12]. Even though tinnitus and dizziness are not always linked to presbycusis, they deteriorate the quality of life of patients who are already severely affected by hearing loss. Risk factors: In our series, high blood pressure and diabetes were found in different proportions, although a large proportion of hypertensive patients had presbycusis. We cannot give a conclusion as to the relationship between these factors and presbycusis. This is because we have not made any statistical correlation calculations. However Rolim LP and al reported in a 2017 study that people with high blood pressure had the greatest decrease in hearing thresholds than people living with diabetes mellitus and those living with high blood pressure combined with diabetes mellitus [13]. In other words, high blood pressure appears to have a greater negative influence on hearing than diabetes mellitus and the combination of high blood pressure and diabetes. According to Cruickshanks and al, cardiovascular risk factors such as smoking, obesity and poorly controlled diabetes are predictive factors for presbycusis [14]. Controlling these factors could therefore delay the onset of deafness [14]. More recent studies have looked for a relationship between heredity and presbycusis. The first findings on the genome, while not conclusive, concluded that the hereditary transmission of presbycusis was overestimated [15]. Alongside these genetic hypotheses, chronic inflammation linked to the ageing process is becoming an increasingly important research topic, and to date several human cohort studies have demonstrated the role of systemic inflammation in presbycusis [16]. Audiometric Aspects: Patients who consult us at the stage of moderate hearing loss are the most representative, at around 51.6%, because at this stage the hearing impairment is greater. Only 10.2% of patients consulted at an early stage. This low rate is due to the fact that mild hearing loss causes the patient listening discomfort only in noise, which is why patients do not feel the need to consult a doctor because they are not very uncomfortable. Severe to profound hearing loss was found in 38.3% of presbycusis patients. These are very hard-of-hearing patients who were diagnosed late; 73% of our patients consulted us between 1 and 10 years. This delay in consulting a hearing aid specialist is linked to patients’ lack of awareness of the possibilities for rehabilitation, and to the high cost of hearing aids. Hearing impairment in the elderly has been shown to be associated with depression and dementia [17]. Early rehabilitation slows the progression of presbycusis and improves the quality of life of these patients [18]. The obstacle of the cost of the hearing aid can be overcome by setting up a program to combat hearing loss. Therapeutic Aspects: During this study, 82.03% of our patients were fitted with a hearing aid. Among them 70.5% noted a clear improvement in hearing even in noise. This demonstrates the effectiveness of hearing aids in presbycusis. However, the cost of the hearing aid is an obstacle to the rehabilitation of presbycusis patients.
Conclusion
Presbycusis is a functional pathology related to aging. Presbycusis will increase at the same time as the life expectancy of our populations. Hearing aids are the mainstay of treatment, but they are expensive, that’s the reason why the public authorities need to get involved.
Data Availability
This patient’s data is recorded in his or her medical file
Conflicts of Interest
The authors declare that they have no conflicts of interest concerning this article
Funding Statement
The authors declare that they have not received any funding Acknowledgments
We thank all person who contributed to this work
References
-
Portmann M, Portmann C (1993) Treatise on Clinical Audiometry. São Paulo, Rock.
-
Wilson DH, Walsh PG, Sanchez L, Davis AC, Taylor AW, et al. (1999) The epidemiology of hearing impairment in an Australian adult population. Int J Epidemiol 28(2): 247-252.
-
Quaranta A, Assennato G, Sallustio V (1996) Epidemiology of Hearing problems among Adults in Italy. Scandinavian audiology Supplementum 42: 9-13.
-
(1996) Audiometric classification of hearing impairments. International Bureau of Audiophonology pp: 1-2.
-
Pearson JD, Morrell CH, Gordon-Salant S, Brant LJ, Metter EJ, et al. (1995) Gender differences in a longitudinal study of age-associated hearing loss. Journal of Acoustical Society of America 97(2): 1196-1205.
-
Jerger J, Chmiel R, Stach B, Spretnjak M (1993) Gender Affects Audiometric Shape in presbyacusis. J Am Acad Audiol 4(1): 42-49.
-
Tenório JP, Guimarães JATL, Flores NGC, Iório MCM (2011) Comparison between classification criteria of audiometric findings in elderly. J Soc Bras Fonoaudiol 23(2): 114-118.
-
(2016) Senegal Population Projection/MEFP/ANSD.
-
Ogunleye AO, Labaran AO (2005) Presbycusis in Nigerians at the University College Hospital, Ibadan. African Journal of Medicine and Medical Sciences 34(3): 293-296.
-
Guincharda AC, Estoppey P, Maire R (2010) Presbyacousie: decrease of the eyes in the aged person. Swiss Medical Forum 17(10): 230-235.
-
Sogebi OA, Olusoga-Peters OO, Oluwapelumi O (2013) Clinical and audiometric features of presbycusis in Nigerians. African Health Sciences 13(4): 886-892.
-
Tan JL, Tang J, Lo S, Yeak S (2016) Investigating the risk factors of vestibular dysfunction and the relationship with presbyacusis in Singapore. J Laryngol Otol 130(9): 816-821.
-
Rolim LP, Samelli AG, Moreira RR, Matas CG, Santos IDS, et al. (2018) Effects of diabetes mellitus and systemic arterial hypertension on elderly patients’ hearing. Brazilian Journal of Otorhinolaryngology 84(6): 754- 763.
-
Cruickshanks KJ, Nondahl DM, Dalton DS, Fischer ME, Klein BEK, et al. (20115) Smoking, Central Adiposity, and Poor Glycemic Control Increase Risk of Hearing Impairment. J Am Geriatr Soc 63(5): 918-924.
-
Bowl MR, Dawson SJ (2019) Age-Related Hearing Loss. Cold Spring Harb Perspect Med 9(8): a033217.
-
Watson N, Ding B, Zhu X, Frisina RD (2017) Chronic Inflammation-inflammaging-In the Ageing cochlea: A novel target for future presbycisus therapy. Ageing Res Rev 40: 142-148.
-
Musiek FE, Rintelmann WF (1999) Current perspectives in hearing assessment. São Paulo.
-
Veras RP, Mattos LC (2007) Audiology and Aging: literature review and current horizons. Braz J Otorhinolaryngol 73(1): 122-128.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?