Endonasal Endoscopic Treatment of Esthesioneuroblastoma
Introduction: Esthesioneuroblastoma is a malignant neoplasm that originates from the olfactory epithelium. Treatment is established according to its extension and the histological degree of atypia and may include surgery, surgery more radiotherapy or more chemoradiation therapy. Different surgical approaches have been used, including facial incisions and craniotomy, but with the greater experience acquired with endoscopic sinus surgery and teamwork with the neurosurgeon, endonasal techniques have been developed that make it possible to perform oncological resections in selected patients, with less morbidity, brief hospitalization and without compromising local control of the disease. Objectives: To determine the rate of local control in patients treated for esthesioneuroblastomas by the endonasal approach with endoscopes or through an endonasal approach with bifrontal craniotomy. Methods: A review of the electronic medical records of patients who were treated for esthesioneuroblastomas in the ENT Department of the Italiano Hospital of Buenos Aires between March 2005 and May 2022 was carried out. Results: Five patients were treated with an endonasal approach with endoscopes. Two patients with an endonasal approach only (Kadish B and C) and three with an endonasal approach combined with bifrontal craneotomy (Kadish C and one D). In four cases, chemotherapy-radiotherapy or radiotherapy was also used. Local control in the treated group was 80% (4/5) and specific survival was 60% (3/5). Conclusions: The local control that we obtained in patients treated for esthesioneuroblastomas through a single endonasal approach or combined with bifrontal craniotomy and adjuvant treatments was 80% and survival without local, regional or distant disease was 60%.
Introduction
Esthesioneuroblastoma (ENB) is a malignant tumor that originates from the olfactory neuroepithelium [1], located in the roof of the nasal cavity, at the level of the upper part of the superior turbinate, nasal septum, and cribriform plate of the ethmoid. From there it can spread and invade the endocranium, paranasal sinuses or orbit [2].
The main treatment is complete surgical resection [3], which can be used as the only modality or in advanced stages, combined with radiotherapy or chemoradiation therapy.
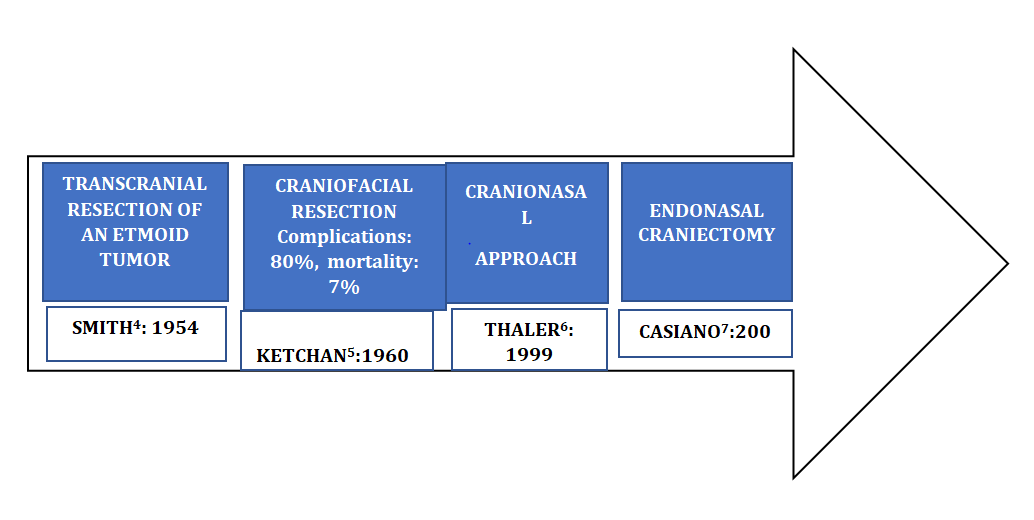
Surgical approaches have evolved from craniofacial surgery to the cranionasal approach or in selected cases, to endonasal craniectomy or hemicraniectomy with endoscopes.
Objectives
To determine the rate of local control in patients treated for esthesioneuroblastomas by the endonasal approach with endoscopes or through an endonasal approach with bifrontal craniotomy.
Design
Descriptive and retrospective
Methods
A review of the electronic medical records of patients who were treated for esthesioneuroblastomas in the ENT Department of the Italiano Hospital of Buenos Aires between March 2005 and May 2022 was carried out.
The following data were collected and analyzed: age, sex, Kadish staging, endonasal surgical technique, adjuvant treatment, complications, local control, and disease-specific survival.
All patients were evaluated by nasal endoscopy, computed tomography (CT) and contrast-enhanced magnetic resonance imaging of the face (MRI), computed tomography of the neck, chest, abdomen, and pelvis, or positron emission tomography (PET).
An endonasal biopsy was performed on all of them prior to treatment, which confirmed the histological diagnosis of ENB.
The therapeutic decision arose from the discussion in
A B
the hospital’s tumor committee.
The surgical approaches used were endonasal only, endonasal combined with a bifrontal craniotomy (cranionasal surgery), and with a Lynch-type incision.
The endonasal surgical technique consisted of resecting a part of the nasal tumor (debulking), in performing a wide medial maxillary antrostomy, anterior and posterior ethmoidectomy, and a bilateral sphenoidotomy with posterior septectomy, using 0º and 30º endoscopes. In one patient an extended Draf II-b frontal sinus drainage was also performed.
When the tumor eroded the medial wall of the orbit, the lamina papyracea and a sector of the periorbita were resected.
The reconstruction of the defect in the anterior skull base in the cases that had an external craniotomy was done using pericranial flaps and in the case in which an endonasal hemicraniectomy was performed, the reconstruction was with a multilayer technique, using synthetic dura mater grafts, abdominal fat, fascia lata and a nasoseptal flap.
Controls were made by nasal endoscopy, CT, MRI and PET.
Results
Five patients were treated, four men and one woman, the mean age was 52.8 years.
Three ENB were staged Kadish C, one B and one D.
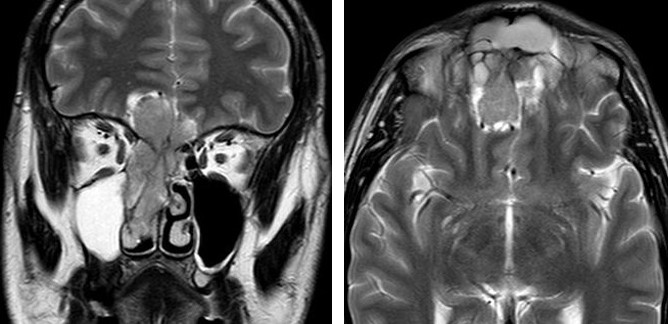
One patient had a history of craniofacial surgery and concurso resect an extension of the tumor in the anterior sector of the medial wall of the orbit (Figure 1).

C D
E F
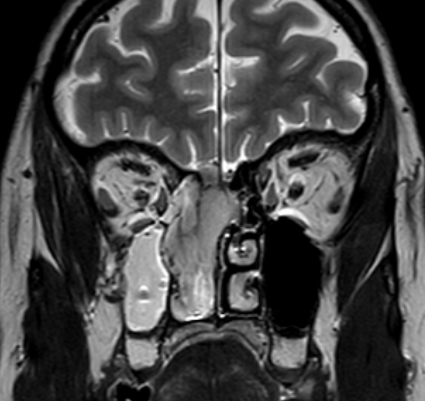
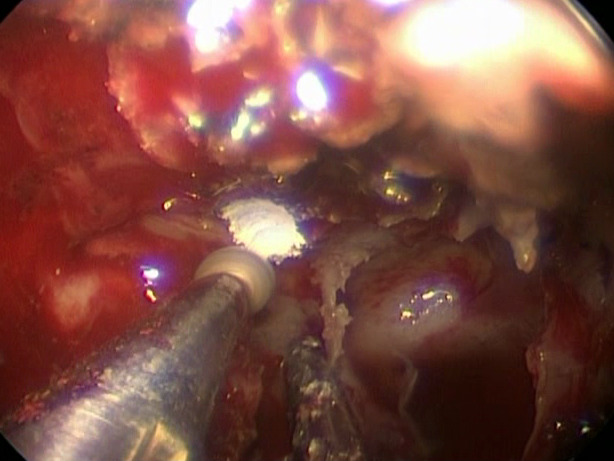
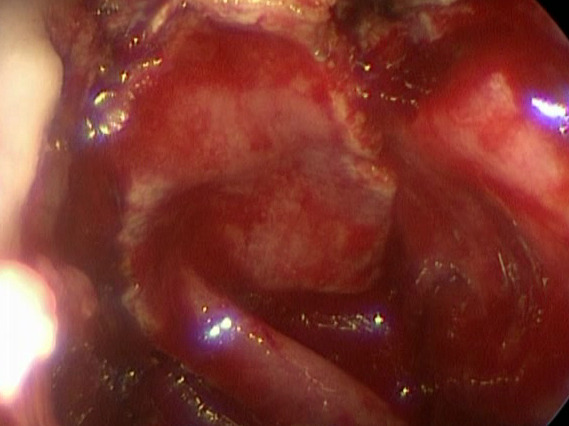
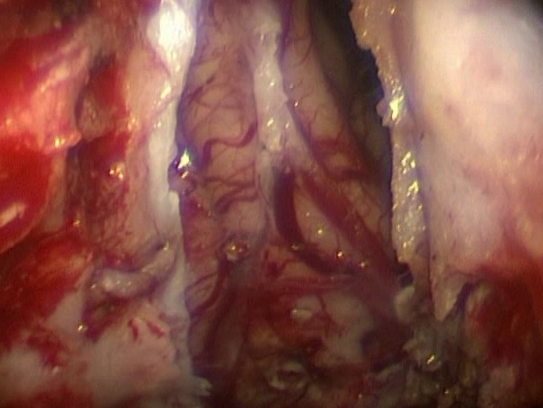
G H Figure 1: Esthesioneuroblastoma Kadish C - A, B: Coronal and Axial MRI Showing the Tumor with Endocranial Extension; C: Endonasal View of the Tumor Surgery; D: Endonasal Resection; E: The Orbit Fat is Observed After Resecting the Periorbita (Black Arrow); F: External Bifrontal Craniotomy (Black Arrow); G: Reconstruction of the Defect with a Pericranial Flap; H: Postoperative CT (Anterior Skull Base Reconstruction with a Pericranial Flap is Observed (Yellow Arrow).
In two, the papyracea lamina and a medial sector of the periorbita were resected.
In a patient with a ENB located in the ethmoids without
bony erosion of the skull base (Kadish B), a wide medial maxillary antrostomy, anterior and posterior ethmoidectomy, median turbinectomy, and resection of the upper septal and orbital mucosa were performed (Figure 2).

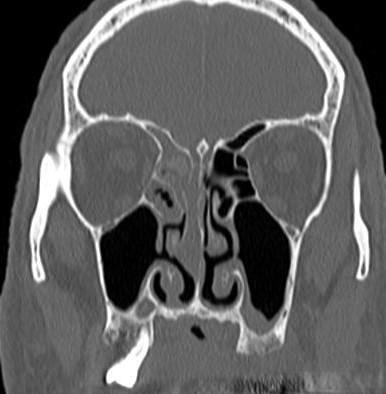
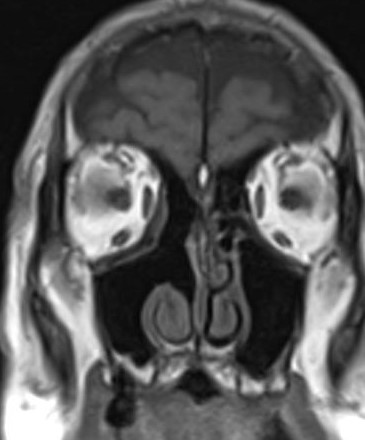
A B C Figure 2: A, B: CT, ENB Located in the Ethmoids without Bony Erosion of the Skull Base is Observed (Kadish B); C: Postoperative MRI.
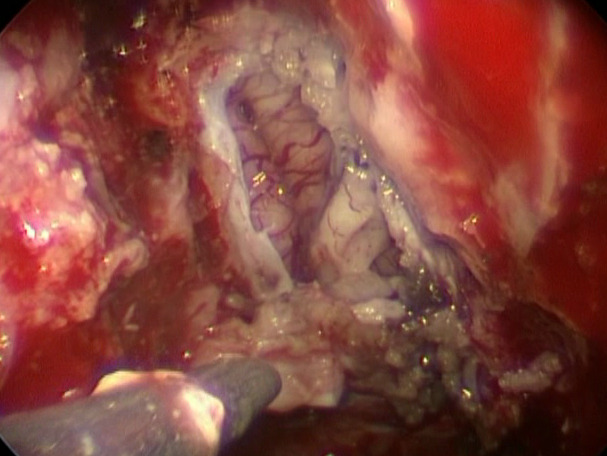
In a patient with a Kadisch C esthesioneuroblastoma, an endonasal hemicraniectomy and multilayer reconstruction with grafts and a nasoseptal flap were performed.
A B C

D E F Figure 3: Esthesioneuroblastoma with Intracranial Extension (Olfactory Bulb) A: MRI (Right Olfactory Bulb Involvement: Arrow). Endonasal Hemicraniectomy – B: Sphenoidotomy; C: Dura Mater Resection with the Tumor (The Olfactory Bulb is Observed: Arrow); D: Endocranial View After Skull Base Resection; E: Multilayer Reconstruction of the Cranial Defect: The Nasoseptal Flap is Observed; F: Postoperative CT.
In all the surgical margins were negative, and were confirmed by intraoperative frozen biopsies, and for the deferred pathological study.
One patient had a dysphonia due to X cranial nerve paralysis of possible viral etiology that recovered spontaneously in 32 days.
Only one patient had a local persistence and two had recurrences in the neck. One had recurrent retropharyngeal and parapharyngeal adenopathies (had been treated prior to surgery for regional disease with CHT+RT), and another had bilateral cervical adenopathies eight years after of the cranionasal surgery.
A bilateral modified radical neck dissection was performed, followed by CHT + reirradiation. The patient lives without local or distant disease.
Local control in the treated group was 80% (4/5) and specific survival was 60% (3/5) (Table 1).
| Age/sex | Kadish | Surgery | Adjuvant treatment | LC | Specific survival | Follow-up |
|---|---|---|---|---|---|---|
| M: 58 | C | cranionasal | preoperative CHT/RT | no | clivus/orbit persistence | 4 years |
| M: 45 | D | cranionasal | preoperative CHT/RT | yes | bilateral retro and parapharyngeal adenopathies | 3 years |
| M: 45 | C | cranionasal | posoperative CHT/RT | yes | yes | 12 years |
| M: 57 | B | endonasal | _ | yes | yes | 3 years |
| F: 59 | C | endonasal hemicraniectomy | posoperative RT | yes | yes | 7 months |
Table 1: Patients Treated for Esthesioneuroblastomas by Endonasal Approach with Endoscopes Alone or by an Endonasal Approach Comb
Discussion
The esthesioneuroblastoma represents between 1% and 5% of malignant tumors of the nasal cavity, and has a bimodal presentation with incidence peaks at 20-30 years and 60-70 years. Surgery is the main therapeutic option in ENB without distant disease.
Surgical approaches have evolved from craniofacial surgery (external paralateronasal or sublabial incision + bifrontal craniotomy) [4, 5], to the combination of endonasal surgery with endoscopes and external craniotomy (cranionasal approach) [6], and even in selected cases to an endonasal craniectomy [7] or hemicraniectomy (Figure 5).
The choice of surgical approach remains a subject of debate. For Kadish A or B stage tumors, an endonasal approach with endoscopes [8] can achieve free margins with a low incidence of complications. However, tumors with lateral supra-orbital extension or extensive dural and brain parenchymal invasion may necessitate a bifrontal craniotomy in conjunction with the endonasal approach [9].
Endonasal surgery is the best therapeutic option to treat located tumors in the nasal cavity.
One case described in this study, an ENB Kadish B, was successfully treated solely with an endonasal approach. The patient experienced a brief hospitalization without complications, achieving local disease control during a 3-year follow-up.
In other patient with a ENB that compromised an olfactory bulb we performed an endonasal hemicraniectomy and were able to resect the tumor with free margins, preserving the contralateral olfactory bulb.
He underwent intensity-modulated radiotherapy, and had no recurrences during the short 7-month Follow-up.
Olfactometry performed 40 days after of the surgery and before starting radiotherapy diagnosed anosmia The short time elapsed since surgery with the presence of nasal crusting and inflammation may possibly have influenced the test result.
In a study involving 22 cases of ENB, an endoscope- assisted endonasal approach was exclusively employed for treatment [10].
Among these cases, 12 patients underwent an endonasal hemicraniectomy to specifically preserve the contralateral olfactory bulb and olfactory function, while 10 patients underwent a bilateral endonasal craniectomy. Successful negative margins were achieved in 21 cases, and no complications were reported.
Following the surgeries, 20 patients received postoperative radiotherapy, ranging between 50 and 60 gray, with 18 cases undergoing intensity-modulated radiotherapy and two receiving conventional RT.
The disease-free survival rate was recorded at 95.5%, with only one patient experiencing a local recurrence at 12 months. The mean follow-up period was 44 months.
In another study Mattavelli D, et al. [11] addressing malignant ethmoid tumors with intracranial invasion, 19 patients underwent endonasal craniectomy using endoscopes, with 11 cases confirming brain invasion through pathology examination. The 3-year survival and local control rates achieved were 65.5% and 81.8%, respectively, and the complication rate was 10.5%.
A meta-analysis, encompassing 609 patients treated for ENB, concluded that endoscopic resection demonstrated a local control rate comparable to craniofacial resection [12].
These results demonstrate the effectiveness of endonasal surgery with endoscopes as a single therapeutic modality or in combination with RT or CHT + RT.
For selected ENB cases, the option of an endonasal hemicraniectomy can be considered, aiming to preserve the contralateral olfactory bulb.
A multicenter study evaluating [13] ENB patient (6 Kadish B, 6 Kadish C, and 2 Kadisch D) treated with surgery plus radiotherapy or radiochemotherapy revealed that the cribriform plate and contralateral olfactory bulb were preserved in all cases. Disease-free surgical margins were obtained, and the smell test conducted approximately 37.3 months after surgery showed residual olfactory function in 43% of patients. No recurrences were reported during a mean follow-up of 51.7 months.
The cranionasal approach was performed in three patients, two were staged Kadish C and one of them had a history of previous treatment with craniofacial surgery and postoperative chemoradiotherapy in another hospital.
Another patient had a Kadish D ENB (bilateral retro and parapharyngeal adenopathies) and was treated prior to cranionasal surgery with CHT + RT with resolution of cervical disease and local persistence.
Local control of the disease was obtained in two patients; the other had a recurrence in clivus.
A meta-analysis encompassing studies from 1990 to 2000 [14], with a 5-year follow-up, reported survival rates of 65% for surgery + radiotherapy, 51% for chemoradiation, 48% for surgery only, 47% for surgery + chemoradiotherapy, and 37% for radiotherapy only. Consistent with other studies Platek ME, et al. [15, 16], the meta-analysis concluded that combined treatment, involving surgery, radiotherapy, and chemotherapy, represents the optimal approach for treating ENB, especially in advanced stages.
Although the incidence of neck metastasis at the time of presentation is uncommon, typically ranging between 5% and 8% [17], some studies reported a higher incidence (12.2%), considering cervical adenopathies as a significant predictor of poor survival [18]. Notably, one patient with ENB Kadish C and another with Kadish D experienced neck recurrences. The former underwent radiotherapy, including cervical fields and chemotherapy before surgery, while the latter developed cervical adenopathies eight years after combined treatment. The neck was treated through a bilateral modified radical neck dissection, followed by CHT + reirradiation.
Zanation AM, et al. [17, 18, 19] recommend elective irradiation of the neck in patients with advanced local stages without cervical disease.
Conclusions
We achieved a local control rate of 80% in patients treated for esthesioneuroblastomas through either a single endonasal approach or a combination with bifrontal craniotomy, along with adjuvant treatments. The survival rate without local, regional, or distant disease was 60%.
The endonasal approach, aided by endoscopes, stands out as the most frequently employed surgical technique for addressing the nasosinusal location of esthesioneuroblastomas.
For Kadish C stage tumors, an endonasal craniectomy or hemicraniectomy can be considered in selected cases. In instances where intracranial invasion is extensive, the endonasal approach with endoscopes may be combined with a bifrontal craniotomy to optimize treatment outcomes.
We do not declare conflicts of interest
References
-
Ward PD, Heth JA, Thompson BG, Marentette LJ (2009) Esthesioneuroblastoma: Results and Outcomes of a Single Institution’s Experience. Skull Base 19(2): 133- 140.
-
Sheehan J, Payne R (2016) Esthesioneuroblastomas. In: Winn HR, Youmans, Winn, Neurological Surgery E-Book. Elsevier Health Sciences, New York, NY, USA, pp: 1284- 1292.
-
Dulguerov P, Allal AS, Calcaterra TC (2001) Esthesioneuroblastoma: a meta-analysis and review. Lancet Oncol 2(11): 683-690.
-
Smith RR, Kloop CT, Williams JM (1954) Surgical treatment of cancer of the frontal sinus and adjacent areas. Cancer 7(5): 991-994.
-
Ketcham AS, Wilkins RH, Van Buren JM, Smith RR (1963) Combined intracranial facial approach to the paranasal sinuses. Am J Surg 106: 698-703.
-
Thaler ER, Kotapka M, Lanza DC, Kennedy DW (1999) Endoscopically assisted anterior cranial skull base resection of sinonasal tumors. Am J Rhinol 13(4): 303- 310.
-
Casiano RR, Numa WA, Falquez AM (2001) Endoscopic resection of esthesioneuroblastoma. Am J Rhinol 15(4): 271-279.
-
Rimmer J, Lund VJ, Beale T, Wei WI, Howard D (2014) Olfactory neuroblastoma: a 35-year experience and suggested follow-up protocol. Laryngoscope 124(7): 1542-1549.
-
Abdelmeguid AS, Raza SM, Su SY, Kupferman M, Roberts D, et al. (2020) Endoscopic resection of sinonasal malignancies. Head Neck 42(4): 645-652.
-
Nakagawa T, Kodama S, Kobayashi M, Sanuki T, Tanaka S, et al. (2017) Endoscopic endonasal management of esthesioneuroblastoma: A retrospective multicenter study. Auris Nasus Larynx 45(2): 281-285.
-
Mattavelli D, Ferrari M, Villaret AB, Schreiber A, Rampinelli V, et al. (2019) Transnasal endoscopic surgery in selected nasal-ethmoidal cancer with suspected brain invasion: Indications, technique, and outcomes. Head Neck 41(6): 1854-1862.
-
Fu TS, Monteiro E, Muhanna N, Goldstein DP, Almeida JRD (2016) Comparison of outcomes for open versus endoscopic approaches for olfactory neuroblastoma: A systematic review and individual participant data meta- analysis. Head Neck 38(Suppl1): E2306-2316.
-
Tajudeen BA, Adappa ND, Kuan EC, Schwartz JS, Suh JD, et al. (2016) Smell preservation following endoscopic unilateral resection of esthesioneuroblastoma: a multi- institutional experience. Int Forum Allergy Rhinol 6(10): 1047-1050.
-
Dulguerov P, Allal AS, Calcaterra TC (2001) Esthesioneuroblastoma: a meta-analysis and review. Lancet Oncol 2(11): 683-690.
-
Platek ME, Merzianu M, Mashtare TL, Popat SR, Rigual NR, et al. (2011) Improved survival following surgery and radiation therapy for olfactory neuroblastoma: analysis of the SEER database. Radiat Oncol 6: 41.
-
Fiani B, Quadri SA, Cathel A, Farooqui M, Ramachandran A, et al. (2019) Esthesioneuroblastoma: A Comprehensive Review of Diagnosis, Management, and Current Treatment Options. World Neurosurg 126: 194-211.
-
Zanation AM, Ferlito A, Rinaldo A, Gore MR, Lund VJ, et al. (2010) When, how and why to treat the neck in patients with esthesioneuroblastoma: a review. Eur Arch Otorhinolaryngol 267(11): 1667-1671.
-
Abdelmeguid AS, Bell D, Roberts D, Ferrarotto R, Phan J, et al. (2022) Long-Term Outcomes of Olfactory Neuroblastoma: MD Anderson Cancer Center Experience and Review of the Literature. Laryngoscope 132(2): 290-297.
-
Jiang W, Mohamed AS, Fuller CD, Kim BYS, Tang C, et al. (2016) The role of elective nodal irradiation for esthesioneuroblastoma patients with clinically negative neck. Pract Radiat Oncol 6(4): 241-247.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?