Inverted Pediatric Sinunasal Papilloma: Case Report
Inverted papilloma (IP) is a rare benign lesion, and only several cases have been described in children. The causes of IP are still unknown. This illness is characterized by a high risk of relapse, also cases of malignancy have been described. Treatment of IP is only surgical. A multi-year period of constant examinations including endoscopy of the nose and sinuses is required after the surgery. In this article, we present a case of inverted papilloma in a 13-year-old boy.
Introduction
Inverted papilloma (IP) is a rare tumor that originates from the epithelial stroma of the mucous membranes of the nose and paranasal sinuses. Although IP is benign, relapses and the risk of malignant transformation are typical for it [1].
Among polypoid formations of the nose and paranasal sinuses, the share of IP is only 0.5-4% [2]. IP is detected mainly in men after the age of 50; the ratio of men to women occurrence is 3:1 [3]. In children, IP is especially rare, with only a few cases described in literature [1]. The first description of pediatric clinical cases of IP includes 3 patients aged 6, 9, and 12 years [4]. In total, less than 20 cases of pediatric IP have been described Topdağ M [5].
IP in children occurs mainly in boys. Those single described cases refer to the age of children from 6 to 15 years. The places of origin of IP there are the maxillary sinuses, nasal septum and middle turbinate [6].
In this article, we present a clinical case of inverted papilloma in a 13-year-old boy.
Patient N., born in 2008, sought help from the Lviv Regional Children’s Clinical Hospital Okhmatdyt in April 2022 with complaints of congestion of the left nostril. These symptoms lasted for the last 6 months. They occurred after the infection of Covid-19. Also discharge with blood impurities occurred 2 weeks ago from the left half of the nose. On examination, the left middle nasal passage is dilated and filled with polypoid masses with a non-smooth granular surface (Figure 1).
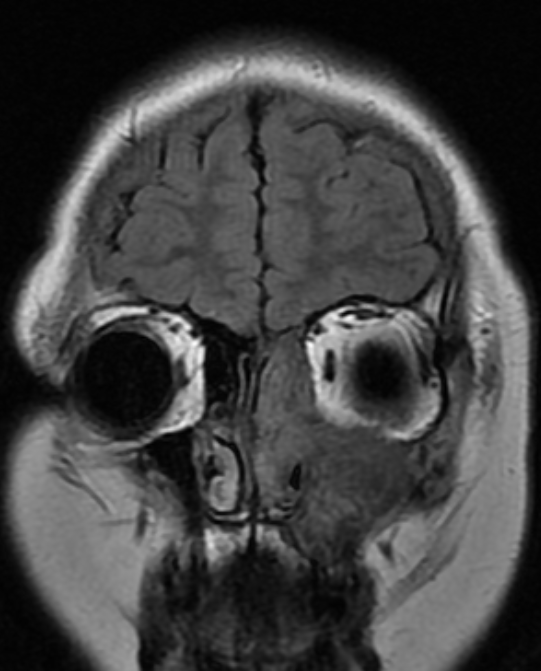
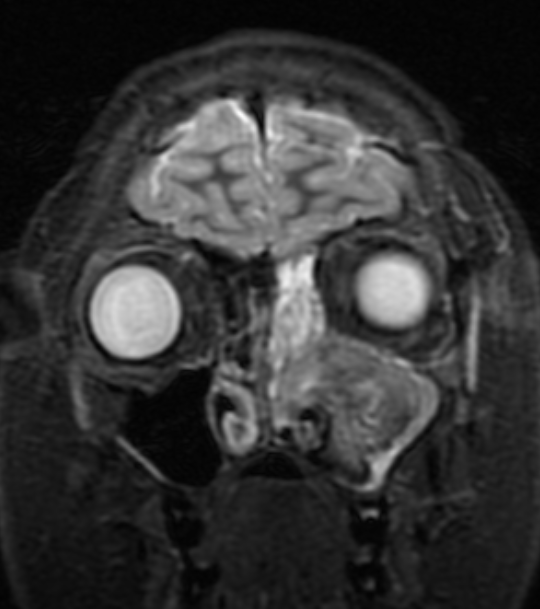
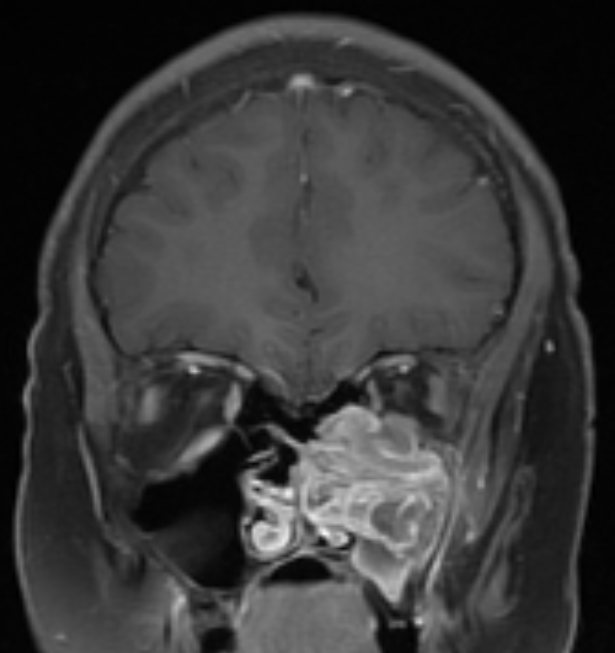
A CT scan of the nose and paranasal sinuses revealed total opacification of the left maxillary and ethmoidal sinuses, and subtotal opacification of the frontal sinus (Figure 2). On the MRI, there is a volumetric formation of the left maxillary sinus, the left half of the nasal cavity, the left ethmoidal labyrinth with expansive growth and deformation of the bone walls of the maxillary sinus (medial displacement of the lateral wall of the sinus, lifting of the inferior wall of the orbit) (Figures 3-5). The radiologist’s conclusion is “volumetric formation of the left maxillary sinus with expansive growth and deformation of the bone walls, the radiological picture may correspond to an inverted papilloma (however, not typical for this age), sinonasal organized hematoma”. A diagnosis of left-sided chronic polyposis pansinusitis with suspicion of inverted papilloma was made and patient was referred to a pediatric ENT department.


In April 2022, an endoscopic wide maxillectomy was performed on the left side, during which it was found that the lesion originated from a limited area of approximately 1 cm2 at the border between the upper and posterior walls of the maxillary sinus in its most lateral part. After removing the lesion from the place of its attachment, there was arterial bleeding, which was stopped by bipolar electrocoagulation. The place of origin of the lesion was also coagulated. Intraoperatively, inflammatory changes with the accumulation of thick mucus were found in the ethmoidal labyrinth and frontal sinus.
Histological conclusion - “the surface of the lesion is covered with multilayered flat epithelium, deep acanthotic strands are formed, which spread into the underlying connective tissue; the composition of cells is normal. The basal membrane is preserved; layers contain a large number of intraepithelial white blood cells; the underlying stroma is sclerosed, there is a diffuse mixed-cell inflammatory infiltrate.
Pathological diagnosis – inverted papilloma with significant inflammatory changes”.
The postoperative period was uneventful. Postoperative consultations during a 9-month period with endoscopy of the left maxillary sinus revealed no recurrence of the papilloma. The patient continues to be under our observation.
Discussion
IP occurs rarely, so the etiopathogenesis of it is not fully elucidated. Possible etiological factors include environmental pollution, allergies, chronic rhinosinusitis, tobacco smoke, and human papillomavirus (HPV-6, HPV-11, HPV-16, HPV- 18) [1]. While taking anamnesis vitae of the patient, it was found that his mother smokes, but according to her, she never smokes at home.
Symptoms of IP in children are identical to other diseases with unilateral localization - unilateral nasal congestion, nasal discharge, possible nosebleeds [6]. When it spreads to neighboring structures other symptoms may occur, such as headache, diplopia, hyposmia, extreme lacrimation. Differential diagnosis includes choanal polyp, hemangioma, encephalocele, mucocele, oncocytic and fungiform papilloma [7].
Histological features of IP in children and adults are identical. IP can coexist with inflammation and inflammatory polyps, so false negative results are reported in up to 17% of cases [8]. Preoperative and postoperative biopsy is required to confirm the diagnosis of IP in adults. Since there is a low risk of malignancy in children, a biopsy may not be performed before surgery [5]. Because of this fact, we did not do a biopsy before the surgery in the described patient.
CT and MRI should be done for preoperative diagnosis. On MRI, IP manifests as unilateral mass of the nose and paranasal sinuses with a convoluted cribriform pattern [9].
IP can be the cause of remodeling or destruction of afferent areas due to compression [5]. To diagnose our patient, we performed both CT and MRI with contrast, which narrowed the range of possible diseases in differential diagnosis and allowed us not to perform a biopsy before surgery.
In the cases described in the literature in children, IP originated from the middle nasal passage and spread to the maxillary sinus [10]. There may occur calcification of the papilloma, as well as thinning or erosion of the bones. The maxillary sinus is most likely involved, although other sinuses can also be affected. IP originated from the maxillary sinus in our patient and caused secondary inflammatory changes in the anterior ethmoidal cells and frontal sinus.
The only method of treatment is surgery, due to the fact, that IP has local aggressive growth and high risk of malignancy [11]. Previously, the “gold standard” was surgery with extranasal approach, but with the development of endonasal endoscopic surgery, minimally invasive methods are more used nowadays. Wide endoscopic access to the maxillary sinus through the middle nasal meatus provides sufficient visualization needed to eliminate IP [12]. We used this technique in our patient too.
In adults, radiation therapy has been described as a method of treatment [13]. It is not recommended for children, since the long-term effects are unknown [5].
Relapses of IP occur in case of incomplete elimination of it because of insufficient visualization of the tumor during surgery. In adults, IP occurs mainly within 6 months after surgery. However, cases of IP recurrence after 20 years have also been described [14]. The frequency of recurrence of IP in adults is 14-78% [1]. Due to the extreme rarity of IP in children, it is impossible to calculate the exact risk of recurrence for them [5]. In two pediatric cases of IP described in literature, relapses were described after 10 and 12 months [15].
Given the high risk of recurrence and the possibility of malignancy, long-term follow-up after surgery is recommended [14]. In order to detect a relapse, endoscopic examination of the nose should be done.
Regular endoscopic examination is mandatory because of the described high risk of recurrence and possible malignant transformation in the period from 1 to 24 years after surgery. A 20-year-old patient in whom IP coexisted with a malignant tumor (low-grade squamous cell carcinoma) is described in literature [4]. We did not find any signs of recurrence in our patient, during 9 months of observation with endoscopic control.
Conclusion
Although IP is extremely rare in children, it should always be taken into account by otorhinolaryngologists in the differential diagnosis of unilateral lesions of the nose and paranasal sinuses in children. Clinical, radiological and histological manifestations of IP in children are identical to those in adults. Treatment of IP in children is exclusively surgical. Since the disease can recur even after a long period of time, periodic postoperative examinations with endoscopy of the nose and sinuses must be performed.
References
-
Jayakody N, Ward M, Wijayasingham G, Fowler D, Harries P, et al. (2018) A rare presentation of a paediatric sinonasal inverted papilloma. J Surg Case Rep 2018(11): rjy321.
-
Cho HJ, Kim JK, Kim KS, Chun JY, Yoon JH (2008) An inverted papilloma isolated to the sphenoid sinus in a pediatric patient. International Journal of Pediatric Otorhinolaryngology Extra 3(3): 124-127.
-
Syrjänen K, Syrjänen S (2013) Detection of human papillomavirus in sinonasal papillomas: systematic review and meta‐analysis. Laryngoscope 123(1): 181- 192.
-
Eavey RD (1985) Inverted papilloma of the nose and paranasal sinuses in childhood and adolescence. Laryngoscope 95(1): 17-23.
-
Topdağ M, Mutlu A, Ila K (2014) Presentation of Childhood Inverted Papilloma with an Antrochoanal Polyp. Turkish Archives of Otolaryngology 52: 106-108.
-
El Korbi A, Jellali S, Kolsi N, Bouatay R, Njim L, et al. (2020) Pediatric naso-sinusal inverted papilloma: report of a case and literature review. Pan Afr Med J 37: 373.
-
Koc C (2013) Nasal Polyp In Can Coc Otorhinolaryngologic Diseases and Head-Neck Surgery, In: 2nd (Edn.), Guneş Tip Kitapevi Ankara, Turkey, pp: 551-68.
-
Lisan Q, Laccourreye O, Bonfils P (2016) Sinonasal inverted papilloma: from diagnosis to treatment. Eur Ann Otorhinolaryngol Head Neck Dis 133(5): 337-341.
-
Kim KR (2001) Inverted papilloma. Journal of Rhinology 8(1-2): 5-10.
-
Ozcan C, Gorur K, Talas D (2005) Recurrent inverted papilloma of a pediatric patient: clinico-radiological considerations. Int J Pediatr Otorhinolaryngol 69(6): 861-864.
-
Ishak MN, Lazim NM, Ismail ZIM, Abdullah B (2019) Open and endoscopic medial maxillectomy for maxillary tumors-a review of surgical options. Curr Med Issues 17(3): 75-79.
-
Pasquini E, Sciarretta V, Farneti G, Modugno GC, Ceroni AR (2004) Inverted papilloma: report of 89 cases. Am J Otolaryngol 25(3): 178-185.
-
Buiret G, Montbarbon X, Fleury B, Poupart M, Pignat JC, et al. (2012) Inverted Papilloma with associated carcinoma of the nasal cavity and paranasal sinuses: Treatment Outcomes. Acta Otolaryngol 132(1): 80-85.
-
D’Angelo AJ, Marlowe A, Marlowe FI, McFarland M (1992) Inverted papilloma of the nose and paranasal sinuses in children. Ear Nose Throat J 71(6): 264-266.
-
Limaye AP, Mirani N, Kwartler J, Raz S (1989) Inverted schneiderian papilloma of the sinonasal tract in children. Pediatr Pathol 9(5): 583-590.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?