Optimizing Visualization and Access to the Maxillary Sinus through the Prelacrimal Approach
Objectives: To determine if endoscopic endonasal prelacrimal approach to the maxillary sinus would be feasible based on the space available between the posterior limit of the frontal process of the maxilla (FPM) at the level of its junction with the anterior wall of the sinus and the anterior wall of the lacrimal duct (NLD) and the rate of complications caused by this approach according to the access space. Material and Methods: Patients who underwent endonasal prelacrimal approach to the maxillary sinus from September 2021 to March 2023 were prospectively evaluated. The distance between the posterior limit of the FPM, at the level of its junction with the anterior wall of the sinus, and the NLD was established on axial cuts of preoperative computed tomography. Three grades were established based on the space between the FPM and the LND: 1) distance less than 3 mm, II) distance between 3 to 7 mm, and III) Distance greater than 7 mm. Results: A total of 30 patients were treated using either a standalone prelacrimal maxillary approach or combined with a medial maxillary antrostomy. There were 5 patients with grade I, 15 with grade II, and 10 with grade III. Only one patient experienced a complication of the approach, transient epiphora for 2 months. In all patients, the prelacrimal approach could be performed without difficulties. Conclusions: The space between the posterior limit of the FPM at the level of its junction with the anterior wall of the sinus and the NLD was not relevant for performing a prelacrimal approach to the maxillary sinus. In cases of reduced prelacrimal windows, the LND was dissected and medialized to perform osteotomy and expose the maxillary sinus. The frequency of complications was 0,3% and was not related to a reduced space (grade 1).
Introduction
The endonasal approach to the maxillary sinus is commonly performed through the middle meatus, following an uncinectomy. Upon identification of the main ostium, its enlargement is undertaken. The size of the medial antrostomy may vary depending on the pathology affecting the maxillary sinus or the need to expose different sectors of the sinus or access adjacent regions. Despite the use of 30-degree endoscopes, visualization of the anterior and anterolateral walls of the maxillary sinus through the medial antrostomy remains limited. In this context, the prelacrimal endonasal approach (PLA) emerges as an alternative that enables adequate exposure of the anterolateral, anteroinferior, and anterosuperior sectors of the maxillary sinus. This allows for the excision of various pathologies located in these areas and, if necessary, can be complemented with a medial maxillary antrostomy.
Objectives
The purpose of this study is to determine the feasibility of the prelacrimal endonasal endoscopic approach to the maxillary sinus, considering the available space between the posterior limit of the frontal process of the maxilla at its junction with the anterior wall of the sinus and the anterior wall of the nasolacrimal duct (NLD). Additionally, we aim to evaluate the rate of complications associated with this approach based on the access space.
Research Hypothesis: Our working hypothesis suggests that a larger space between the frontal process of the maxilla and the anterior wall of the lacrimal nasolacrimal duct would facilitate the prelacrimal endonasal approach to the maxillary sinus. In other words, it is posited that the breadth of this space could positively influence the feasibility and safety of the intervention, reducing potential complications arising from the procedure. Design Prospective and descriptive.
Materials and Methods
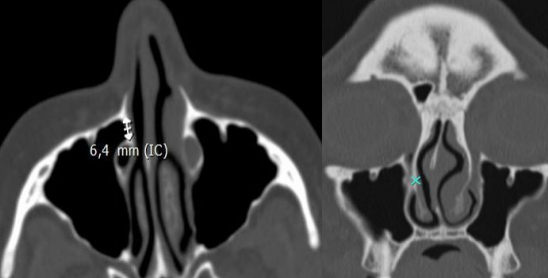
The evaluation included patients undergoing a prelacrimal endonasal approach to the maxillary sinus between September 2021 and March 2023. Prospective data were recorded in an Excel spreadsheet, including information on patients’ age and sex, treated pathology, distance between the posterior limit of the maxillary ascending process to the lacrimal nasolacrimal duct, difficulty experienced in accessing the maxillary sinus, and complication rate. The measurement of the distance between the posterior limit of the frontal process of the maxilla at its junction with the anterior wall of the sinus and the lacrimal nasolacrimal duct was performed on preoperative computed tomography axial slices. The measurement was conducted using the measurement tool in the Alma m CLINIC Dicom Study Manager program. It was performed on the lowest coronal slice where the nasolacrimal duct was observed, coinciding with the insertion of the turbinate bone into the frontal process of the maxilla (Figure 1).
The space between the FPM and the NLD was classified into three grades:
- Grade I: distance less than 3 mm.
- Grade II: distance between 3 to 7 mm.
- Grade III: distance greater than 7 mm.
The surgical technique was performed under general anesthesia on an outpatient or inpatient basis, depending on the anesthetic surgical risk and the complexity of the pathology. 0-degree endoscopes, chisels, hammer, and conventional instrumentation for endoscopic paranasal sinus surgery were used. Prior to the procedure, cotton balls soaked in lidocaine and adrenaline 1/100,000 were applied without infiltrating the lateral wall. The incision, made with a cautery, was 3 mm in length anterior to the head of the inferior turbinate, from the superior sector of the turbinate to the nasal floor, with an intensity of 15 and in cutting and coagulation mode. The surgical technique involved dissecting the medial wall of the maxillary sinus from the frontal process of the maxilla backward in a subperiosteal plane, displacing the inferior turbinate and the lacrimal duct medially in its anterior sector. The medial bony wall of the sinus was exposed in the inferior meatus in its anterior sector, and an anterior antrostomy was performed using chisels while preserving the frontal process of the maxilla. If necessary, the antrostomy was enlarged using Blackesley or Kerrison forceps. The size of the prelacrimal antrostomy varied depending on the treated pathology and the need to expose different sectors of the maxillary sinus or the pterygopalatine fossa, which could be combined with a medial maxillary antrostomy. During the surgery, adequate visualization of the anterior, lateral, anterosuperior, and anteroinferior walls of the maxillary sinus was achieved.
Upon completion, the inferior turbinate was sutured to the lateral nasal wall with one or two absorbable sutures (3/0 Vicryl). A hemostatic matrix (Surgiflo) was applied, and in cases of associated septoplasty, a silicone splint was placed and removed after 10 days (Figure 2).
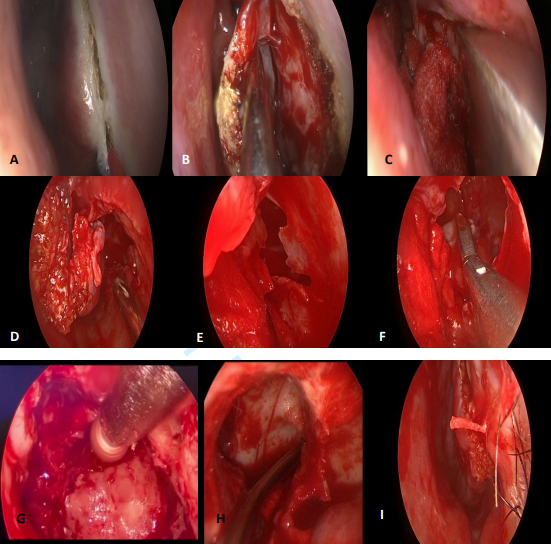
Figure 2: Prelacrimal Endonasal Approach to the Maxillary Sinus with Endoscopes. A: Incision with Cautery 3mm Anterior to the Inferior Turbinate; B: Subperiosteal Dissection; C: Prelacrimal Maxillary Osteotomy with Chisel; D,E: Prelacrimal Maxillary Window; F: Resection with Forceps of an Inverted Papilloma with Anteroinferior Implantation; G: Milling of the Maxillary Sinus through the Prelacrimal Window; H: Endoscopic View of the Anterior, Inferior, an Lateral Sectors of the Maxillary Sinus After Milling the Site of Inverted Papilloma Implantation; I: Suturing of the Inferior Turbinate.
Results
A total of 30 patients were included in the study, comprising 20 males and 10 females, with an average age of 52.86 years (range: 17 to 82 years). The diseases affecting the maxillary sinus were diverse and classified into inflammatory and benign/malignant tumor categories:
Inflammatory Diseases
- Antrochoanal polyp (8/30).
- Chronic sinusitis (2/30).
- Foreign body in the maxillary sinus (1/30).
- Allergic fungal rhinosinusitis (2/30).
- Fungal ball (2/30).
- Mucocele (1/30).
- Odontogenic cysts (2/30).
Benign Tumors
- Thrombosed hemangioma (1/30).
- Inverted papillomas (7/30).
- Angiofibroma (1/30).
Malignant Tumors
- NK lymphoma (1/30).
- Epidermoid carcinoma with metachronous inverted papilloma (1/30).
- Low-grade mucoepidermoid carcinoma (1/30).
Based on the space identified in the axial slice of the computed tomography between the posterior aspect of the superior maxillary ascending process and the anterior wall of the nasolacrimal duct, it was observed that 5 patients had grade I (7 mm). In all cases, the prelacrimal approach was successfully performed without complications, even in those patients with an access space less than 3 mm (grade I).
Only one complication of the prelacrimal approach was recorded, consisting of transient epiphora affecting a single patient for 2 months, whose FPM-NLD distance was 3.78 mm (grade II) (Table 1).
| N | Age/Sex | Pathology | Distance between FPM and LD | Type of maxillary approach | Difficulty to maxillary access | Complications from the prelacrimal approach |
|---|---|---|---|---|---|---|
| 1 | F/17 | right antrochoanal polyp | grade III | prelacrimal | no | no |
| 2 | M/58 | right antrochoanal polyp | grade II | prelacrimal + medial maxillary antrostomy | no | no |
| 3 | M/47 | left antrochoanal polyp | grade II | prelacrimal | no | no |
| 4 | F/17 | left antrochoanal polyp | grade III | prelacrimal | no | no |
| 5 | M/29 | left antrochoanal polyp | grade II | prelacrimal + medial maxillary antrostomy | no | no |
| 6 | F/63 | left antrochoanal polyp | grade II | prelacrimal | transient epiphora | |
| 7 | F/50 | left antrochoanal polyp | grade II | prelacrimal + medial maxillary antrostomy | no | no |
| 8 | M/29 | right antrochoanal polyp | grade III | prelacrimal | no | no |
| 9 | F/69 | chronic sinusitis | grade III | prelacrimal + medial maxillary antrostomy | no | no |
| 10 | F/80 | left hyperplastic sinusitis | grade I | prelacrimal + medial maxillary antrostomy | no | no |
| 11 | M/42 | allergic fungal rhinosinusitis | grade III | prelacrimal + medial maxillary antrostomy | no | no |
| 12 | M/18 | allergic fungal rhinosinusitis | grade II | prelacrimal + medial maxillary antrostomy | no | no |
| 13 | M/67 | left fungal ball | grade III | prelacrimal + medial maxillary antrostomy | no | no |
| 14 | F/82 | left fungal ball | grade II | prelacrimal + medial maxillary antrostomy | no | no |
| 15 | M/72 | mucocele | grade I | prelacrimal + medial maxillary antrostomy | no | no |
| 16 | M/12 | left odontogenic cyst | grade III | prelacrimal + medial maxillary antrostomy | no | no |
Table 1: Patients Treated Using a Prelacrimal Approach to the Maxillary Sinus FPM: Frontal Process of the Maxilla; NLD: Lacrimona
- 17
- M/45 left odontogenic cyst grade II prelacrimal + medial maxillary antrostomy no no
- 18
- M/73 maxillary foreign body grade III prelacrimal + medial maxillary antrostomy no no
- 19
- M/70 right maxillary thrombosed hemangioma grade III prelacrimal + medial maxillary antrostomy no no
- 20
- F/72 inverted papilloma
- + left allergic fungal rhinosinusitis grade II prelacrimal + medial maxillary antrostomy no no
- 21
- M/51 left maxillary inverted papilloma grade I prelacrimal + medial maxillary antrostomy no no
- 22
- M/52 left maxillary inverted papilloma grade I prelacrimal + medial maxillary antrostomy no no
- 23
- F/69 left maxillary inverted papilloma grade II prelacrimal no no
- 24
- M/67 left maxillary inverted papilloma grade II prelacrimal + medial maxillary antrostomy no no
- 25
- M/68 left maxillary inverted papilloma grade II prelacrimal + medial maxillary antrostomy no no
- 26
- M/66 left maxillary inverted papilloma grade II prelacrimal + medial maxillary antrostomy no no
- 27
- M/17 angiofibroma grade II prelacrimal + medial megaantrostomy no no
- 28
- F/47
- NK lymphoma (biopsy) grade II prelacrimal + medial maxillary antrostomy no no
- 29
- F/78 low-grade mucoepidermoid carcinoma (biopsy) grade III prelacrimal no no
- 30
- M/59 maxillary squamous cell carcinoma with inverted papilloma (biopsy) grade I prelacrimal no no
Table 2: Patients Treated Using a Prelacrimal Approach to the Maxillary Sinus FPM: Frontal Process of the Maxilla; NLD:
During postoperative follow-ups, the presence of a fibrin plug obstructing nasal cavity between the septum and the inferior turbinate in its anterior sector was observed in the majority of patients. This plug required removal via aspiration and forceps to ensure adequate nasal patency and facilitate the patients’ recovery process.
Discussion
Different endonasal approaches with endoscopes to the maxillary sinus exist, varying in their degree of invasiveness and extension. These include uncinectomy without manipulation of the maxillary ostium, considered a form of minimal endoscopic surgery.
Also mentioned is the medial maxillary antrostomy, with the possibility of enlarging the natural ostium to achieve mega-antrostomy, extending from the pterygoid process to the lacrimal duct, while preserving it [1]. These approaches adequately expose the medial and posterior sectors of the maxillary sinus. However, achieving complete visualization of the anterior, anterolateral, anterosuperior, and anteroinferior walls is noted to be challenging, even with the use of 30-degree optics. Extended approaches are also mentioned, such as medial maxillectomy, involving a medial maxillary antrostomy from the pterygoid process to the frontal process of the maxilla. This procedure includes cauterization of the sphenopalatine artery, sectioning of the lacrimal duct, and resection of the inferior turbinate [2].
Another extended approach is the endoscopic Denker, involving the resection with a drill of the frontal process of the maxilla and part of the anterior wall of the maxillary sinus. These extended approaches allow visualization of the anterior sector of the maxillary sinus but are associated with increased morbidity.
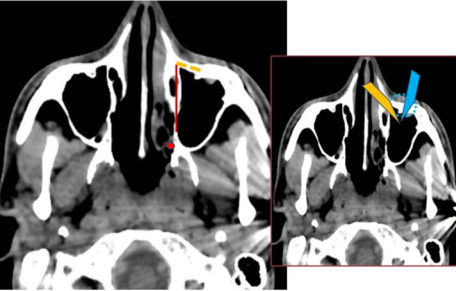
The risk of developing empty nose syndrome is mentioned Chen XB, et al. [3], as well as the possibility of functional and aesthetic alterations, including collapse of the nasal wing due to the absence of the frontal process of the maxilla [4] (Figure 3).
The sublabial route offers another alternative to access the maxillary sinus through an anterior sinusotomy.
However, the prelacrimal approach, introduced by Zhou B, et al. [5] and primarily used in patients with inverted papillomas in Krouse stages T3-5, has gained relevance [6]. Studies based on tomography have revealed significant variability in the anatomy of the prelacrimal space. Kashlan K, et al. [7] reported that the anteroposterior dimension of the prelacrimal space is larger in its inferior sector, with a mean of 8.4 mm and a range of 1.9 mm to 14.2 mm, while the height varied between 18.5 mm and 39.9 mm.
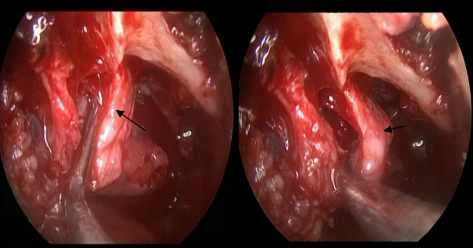
Another study by Sieskewicz A, et al. [8] found that the width of the prelacrimal recess at the level of the inferior turbinate ranged from 0 to 15.2 mm, and in 30% of the studied patients, the space was too narrow to allow passage of a 4 mm endoscope. Simmen D, et al. [9] analyzed computed tomography scans of the paranasal sinuses, measuring the distance between the anterior wall of the maxillary sinus and the anterior border of the lacrimal duct (prelacrimal window). They classified the prelacrimal space into three grades: < 3 mm (grade 1), 3 to 7 mm (grade 2), and > 7 mm (grade 3). They described a frequency of 31.5% for grade 1, 56.5% for grade 2, and 12.5% for grade 3. They concluded that only in 12.5% of cases is it possible to perform a prelacrimal approach without difficulties, and in the rest, dislocation of the lacrimal sac may be necessary. In this study, we observed that it was more frequent to find a prelacrimal space between 3-7 mm (grade 2) in 51.72%, followed by a distance greater than 7 mm (grade 3) in 31.03%, and a distance less than 3 mm (grade 1) in 17.24%. The smaller prelacrimal window did not affect the approach, as we medially displaced the mucoperiosteum of the lateral wall with the anterior sector of the inferior turbinate, dissecting and medializing the lacrimal duct to perform the osteotomy. Ashman A, et al. [2] concluded that a reduced distance (<3 mm) between the frontal process of the maxilla and the lacrimal duct would not contraindicate the prelacrimal approach, as the lacrimal duct can be dissected and medialized to allow for the osteotomy (Figure 4).
Morrisey DK, et al. [10] modified the prelacrimal approach by associating it with a maxillary antrostomy in the middle meatus, resecting 3 mm of the piriform aperture.
However, in this study, it was preferred not to partially or totally resect the piriform aperture. The osteotomy was performed on the lateral bony wall behind the PA, achieving adequate visualization of the most anterior sectors in all cases.
In 22 out of 29 patients, a middle meatal maxillary antrostomy was associated with the prelacrimal approach. Surgery started with the middle meatal maxillary antrostomy, and if the anterior-inferior, anterior-superior, or anterolateral sectors of the maxillary sinus were not adequately visualized, the prelacrimal antrostomy was performed.
In cases of antrochoanal polyps with anterior implantation, the prelacrimal approach alone was sufficient to resect the polyp and curette or drill the implantation site in four treated patients. In odontogenic cysts or benign tumors, it was considered preferable to associate medial antrostomy with the prelacrimal approach (PLA) to fully expose and resect the lesions. For other tumors, the PLA offered greater exposure and a wider angle of vision of neighboring regions such as the pterygopalatine fossa or infratemporal region. In cases of malignant tumors with a more anterior localization, the PLA was used to obtain a biopsy for histopathological study, thus avoiding an anterior maxillary sinusotomy.
In Zhou B, et al. study [5], a 7% rate of paresthesia in the upper lip or nasal wing and a 5.6% rate of mild alar collapse were observed in 71 patients treated for inverted papillomas using the prelacrimal access. It is important to note that 8 patients underwent partial osteotomy of the frontal process of the maxilla at the piriform aperture. In our approach, we chose not to perform osteotomy in the frontal process of the maxilla. Instead, we entered the maxillary sinus behind this structure and adequately exposed the anterolateral, anteroinferior, and anterosuperior regions.
In another study involving 40 patients treated using a prelacrimal approach [11], early paresthesia was reported in 10% and late paresthesia in 2.5%. In our series of cases, no patients reported postoperative paresthesias, possibly due to the preservation of the frontal process of the maxilla. The incidence of complications were low, with only one patient experiencing epiphora (4.16%), which was associated with a distance of 3.78 mm between the frontal process of the maxilla and the lacrimal duct (grade 2). This suggests that the implemented prelacrimal approach was associated with a low complication rate.
Conclusions
The study concluded that the space between the posterior limit of the frontal process of the maxilla, at the level of its junction with the anterior wall of the sinus, and the lacrimal duct was not a determining factor for successfully performing a prelacrimal approach to the maxillary sinus. In situations were reduced prelacrimal windows existed, the option was chosen to dissect the lacrimal duct and medially displace it to facilitate osteotomy and exposure of the maxillary sinus.
It is noteworthy that the frequency of complications was low, specifically 0.3%, and no relationship was found with the reduction of space (grade 1). These findings suggest that the prelacrimal approach to the maxillary sinus is a safe and effective technique, even in conditions where space is limited.
Conflict of Interest Statement
We declare no conflicts of interest.
References
-
Sommer F, Hoffmann T, Lindemann J, Hahn J, Theodoraki MN (2020) Radicality of maxillary sinus surgery and size of the maxillary sinus ostium. HNO 68(8): 573-580.
-
Ashman A, Psaltis AJ, Wormald PJ, Tan NC-W (2020) Extended endoscopic approaches to the maxillary sinus. The Journal of Laryngology & Otology 134(6): 473-480.
-
Chen XB, Leong SC, Lee HP, Chong VF, Wandy DY (2010) Aerodynamic effects of inferior turbinate surgery on nasal airflow - a computational fluid dynamics model. Rhinology 48(4): 394-400.
-
Bertazzoni G, Accorona R, Schreiber A, Pietrobon G, Karligkiotis A, et al. (2017) Postoperative long-term morbidity of extended endoscopic maxillectomy for inverted papilloma. J Rhinol 55(4): 319-325.
-
Zhou B, Han D, Cui SJ, Huang Q, Wang CS (2013) Intranasal endoscopic prelacrimal recess approach to maxillary sinus. Chin Med J 126(7): 1276-1280.
-
Zhou B, Huang Q, Sun J, Li X, Zhang W, et al. (2018) Resection of inverted papilloma of the maxillary sinus via a prelacrimal recess approach: a multicenter retrospective analysis of surgical efficacy. Am J Rhinol Allergy 32(6): 518-525.
-
Kashlan K, Craig J (2018) Dimensions of the medial wall of the prelacrimal recess. Int Forum Allergy Rhinol 8(6): 751-755.
-
Sieskiewicz A, Buczko K, Janica J, Lukasiewicz A, Lebkowska U, et al. (2017). Minimally invasive medial maxillectomy and the position of nasolacrimal duct: the CT study. Eur Arch Otorhinolaryngol 274(3): 1515-1519.
-
Simmen D, Veerasigamani N, Briner HR, Jones N, Schuknecht B (2017) Anterior maxillary wall and lacrimal duct relationship - CT analysis for prelacrimal access to the maxillary sinus. Rhinology 55(2): 170-174.
-
Morrissey DK, Wormald PJ, Psaltis AJ (2016) Prelacrimal approach to the maxillary sinus. International Forum of Allergy & Rhinology 6(2): 214-218.
-
Seresirikachorn K, Kondo M, Png LH, Kalish L, Campbell RG, et al. (2022) Prelacrimal Approach to Maxillary Sinus Pathology. Am J Rhinol Allergy 37(3): 369-373.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?