Utility of the Retroauricular Island Flap for Squamous Cell Carcinoma Reconstruction in the Concha: A Case Study
In a clinical case, we illustrate the usefulness of the retroauricular revolving door island flap (RDIF) described for the first time by Masson JK in 1972 [1], to reconstruct large defects of the auricular concha, with the aim of spreading its knowledge in the field of Otorhinolaryngology.
Abbreviation
RDIF: Retroauricular Revolving Door Island Flap.
Introduction
Reconstruction of the pinna is a challenge for the specialist, as it is a visible area, with thin skin and cartilaginous support, which must be symmetrical and there is always a risk of necrosis due to being located in a distal area of the body.
Defects in this area, can have different etiologies: traumatic, congenital, infectious, oncological, etc. There are different reconstruction options described, for example, the preauricular translocation flap, only for defects that are in the lower part of the concha and less than 15 mm in diameter [2].
For this reason, we present this case in which a versatile flap, with a single surgical stage, useful on large defects, was used.
Clinical Note
Clinical Case
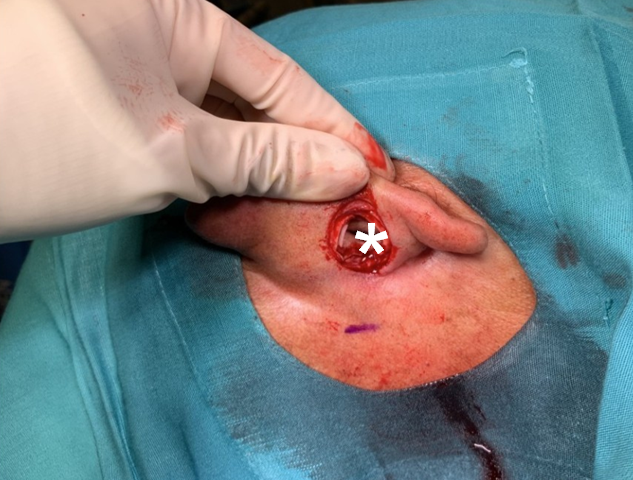
An 80-year-old male presented with a right retroauricular lesion, at the level of the concha, of 7 months’ duration, who had received medical treatment on several occasions based on antibiotics and analgesics. The lesión was approximately 1.5 cm in diameter and caused pain, presented exudate and was recently increased in diameter (Figure 1).
A biopsy was taken from the edges of the lesion and the pathological anatomy results reported dermal infiltration by squamous cell carcinoma (p40 positive).
Due to the patient’s history: dilated cardiomyopathy, bilateral complete occlusion of superficial femoral artery, recanalization of popliteal arteries, prostate cancer, left nephrectomy for renal adenocarcinoma during which splenectomy was performed in the context of a surgical complication (perinephric hematoma spontaneous), right inguinal radical orchiectomy, recent nodular-cystic basal cell carcinoma in vertex nasal and reconstruction with plasty using a frontonasal flap with pedicle in the nasalis muscle; it was decided to perform the resection under local anesthesia.


2. Rotation of the island flap was performed (Figure 4)

3. Reconstruction was carried out with simple non-absorbable sutures (Figure 5 & 6)


4. Stitches were removed a week, finding the flap in excellent condition and the patient was reviewed a month and a half after surgery (Figures 7 & 8)


The final pathology report was:
- Compatible with moderately differentiated and infiltrating squamous cell carcinoma.
- Tumor size: 1.5 cm maximum dimension.
- Deep tumor invasion: 7 mm, by immunohistochemical study (p40), with lower edge in contact with the lesion, rest of edges free.
Due to the result, the case was discussed with the hospital’s tumor committee, recommending complementary radiotherapy, which the patient will begin as soon as possible.
Discussion
In the seventh classification of the American Joint Committee on Skin Cancer, two high- risk anatomical locations have been specified: the lip and the pinna. The proportion of cutaneous squamous cell carcinoma that metastasize is usually 2-6%, but in these locations, it increases to 14-16% [3], thus worsening the stage [3]. It was classically attributed to the fact that they are richly innervated and vascularized areas, with little subcutaneous tissue, which would facilitate the invasion of deep structures and rapid dissemination.
Specifically, retroauricular concha squamous carcinomas are not frequent and the reconstruction of defects in the concha, both anteriorly and posteriorly, is a challenge due to complex topography, the reduced skin laxity and the difficult access surgical of the area. There are surgical alternatives, such as the preauricular translocation flap [2].
The RDIF was described by first time in 1972 by Masson JK [1] and we specify the steps with the images.
The anterior zone of the pinna receives vascularization from the superficial temporal artery that emits 2-3 anterior auricular arteries and the retroauricular area receives vascularization from the posterior auricular artery that includes perforating branches, so that both territories, anterior and posterior, anastomose completely. In addition, a vascular arcade is formed in the auriculo-cephalic sulcus, creating a territory of great superficial and deep irrigation [4].
The RDIF favors the closure of large defects in an only surgical time, up to 3 cm in diameter, with minimal risk of necrosis [5]. In fact, the greatest diameter of the excised area allows for more thickness in the pedicle and a tunnel with an increase in diameter, which favors the flap vitality and ensures oncological margins [6].
It also has the advantage that the retroauricular skin is lax and of the same color as the skin of the anterior region, which makes it easier to hide the scar. As a disadvantage we could mention that retroauricular area is a surgical field with difficult visualization.
This flap has also been used with good results in the reconstruction of the triangular and scaphoid fossa [7].
Conclusion
This flap is a versatile option for the reconstruction of anterior and posterior ear defects, with a high success rate and we must keep it in mind in our surgical arsenal.
References
-
Masson JK (1972) A simple island flap for reconstruction of concha-helix defects. Br J Plast Surg 25: 399-403.
-
Zhu J, Zhao H, Wu K, Lv C, Bi HD, et al. (2016) Reconstruction of auricular conchal defects with local flaps. Medicine (Baltimore) 95(46): e5282.
-
Farasat S, Yu SS, Neel VA, Nehal KS, Lardaro T, et al. (2011) A new American Joint Committee on Cancer staging system for cutaneous squamous cell carcinoma: creation and rationale for inclusion of tumor (T) characteristics. J Am Acad Dermatol 64(6): 1051-1059.
-
Pinar YA, Ikiz ZA, Bilge O (2003) Arterial anatomy of the auricle: its importance for reconstructive surgery. Surg Radiol Anat 25(3-4): 175-179.
-
Krespi YP, Ries WR, Shugar JM, Sisson GA (1983) Auricular reconstruction with postauricular myocutaneous flap. Otolaryngol Head Neck Surg 91(2): 193-196.
-
Redondo P, Lloret P, Sierra A, Gil P (2003) Aggressive tumors of the concha: treatment with postauricular island pedicle flap. J Cutan Med Surg 7(4): 339-343.
-
Dyson ME, Orangi M, Goldberg LH, Kimyai-Asadi A (2019) Repair of Anterior Ear Defects Using Transcartilage Island Pedicle Flaps. Dermatol Surg 45(10): 1222-1227.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?