Sphenoid Sinus Inverted Papilloma: A Rare Presentation and Treatment Challenges
Inverted papilloma is a benign tumor that can undergo synchronous or metachronous malignant transformation. Its isolated location in the sphenoid sinus is rare and its surgical treatment is challenging due to the anatomical variants that may exist and the nervous and vascular structures that are related to this sinus. Objectives: To determine the local control rate in inverted papillomas and synchronous carcinomas with inverted papilloma located in the sphenoid sinus, and to describe the surgical technique for inverted papillomas according to the anatomical characteristics of the sphenoid. Methods: Patients who were evaluated and treated for inverted papillomas primarily located in the sphenoid sinus from 2002 to 2023 in the Rhinosinusology and Skull Base Section of the ENT Department at the Hospital Italiano de Buenos Aires were included. A nasal corridor was created by resecting the middle turbinate in some patients, and anterior and posterior ethmoidectomies with unilateral maxillary antrostomy were performed, choosing the most affected nasal cavity by the tumor. Next, a posterior septectomy was done to expose the entire sphenoid from one nasal fossa. The inverted papilloma was then resected, starting from the center to induce a central collapse, followed by excision of the lateral remnants in contact with the carotid artery and optic nerve. In patients with sphenoid sinuses with pneumatization of the pterygoid processes and highly developed lateral recesses, the trans-pterygoid endonasal approach was combined with sphenoidotomy In inverted papillomas with synchronous squamous carcinomas, treatment with cisplatin and intensity-modulated radiation therapy (IMRT) was associated with the biopsy or debulking. Follow-up was performed through nasal endoscopy magnetic resonance imagen. Results: Six patients were treated: five males and one female, with inverted papillomas mainly located in the sphenoid sinus. Two of them had synchronous squamous carcinomas. In one patient, subtotal resection was performed as the intraoperative biopsy was reported as inflammatory tissue. After the final diagnosis of inverted papilloma, the patient refused further surgery The final local control rate we achieved in three patients treated through endonasal approaches with endoscopes for curative purposes was 66.66%. Local control in synchronous carcinomas with inverted papilloma staged as T4-b was 50%. Conclusions: The final local control rate we achieved in three patients treated through endonasal approaches with endoscopes for curative purposes was 66.66%. Local control in synchronous carcinomas with inverted papilloma staged as T4-b was 50%. The main endonasal technique is wide paraseptal sphenoidotomy. We prefer to perform a central resection of the tumor and then dissect the lateral walls of the sinus. In cases of extensive pneumatization of the sphenoid and the presence of lateral recesses, we believe it is better to combine sphenoidotomy with a trans-pterygoid approach.
Abbreviations
IP: Inverted Papilloma; MRI: Magnetic Resonance Imagen; CT: Computed Tomography.
Introduction
Inverted papilloma (IP) is a benign tumor that originates from the mucosa of the nasal cavities and paranasal sinuses. It is characterized by its local aggressiveness, tendency to recur, and potential for malignancy.
The epithelium exhibits an inverted growth pattern, invaginating and growing into the underlying stroma, but the basement membrane remains intact. Most cases involve the mucosa of the nasal cavity and paranasal sinuses, with isolated involvement of a paranasal sinus being rare (0.5%).
Isolated involvement of the sphenoid sinus is very rare, and complete tumor resection is challenging due to the possibility of the lesion eroding bone and extending into adjacent vital structures such as the optic nerve, oculomotor nerves, and internal carotid artery.
Additionally, anatomical variants of the sphenoid, such as excessive pneumatization with wide lateral recesses, dehiscences of the internal carotid artery, optic nerve, or bony septa connected to the second cranial nerve or the carotid artery, may increase the difficulties of surgical resection and complications.
Objectives
To determine the local control rate in inverted papillomas and synchronous carcinomas with inverted papilloma located in the sphenoid sinus, and to describe the surgical technique for inverted papillomas according to the anatomical characteristics of the sphenoid.
Design
Descriptive and retrospective.
Materials and Methods
Patients who were evaluated and treated for IP primarily located in the sphenoid sinus from 2002 to 2023 in the Rhinosinusology and Skull Base Section of the ENT Department at the Hospital Italiano de Buenos Aires were included. The following data were collected in an Excel table they are sex and age of the patients, presenting symptoms, imaging characteristics, endonasal surgical technique, histopathology, and treatment outcomes and follow-up. All patients were evaluated through otorhinolaryngological examination, nasal endoscopy, non-contrast facial computed tomography scan (CT), and contrast-enhanced facial magnetic resonance imagen (MRI). In nearly all patients, a prior biopsy of the lesion was performed via the endonasal approach. The IP involving the sphenoid sinus were staged according to Krouse as grade III, and synchronous squamous carcinomas were staged Krouse IV [1] and according to the AJCC classification of 2017, 8th edition, as T4-B (Table 1).
| Stage | |
|---|---|
| T1 | Tumor isolated to one area of the nasal cavity without extension to the paranasal sinuses |
| T2 | Tumor involves medial wall of the maxillary sinus, ethmoid sinuses or osteomeatal complex |
| T3 | Tumor involves the superior, inferior, posterior, anterior, or lateral wall of the maxillary sinus, frontal sinus, or sphenoid sinus |
| T4 | Tumor with extrasino nasal extent or malignancy |
Table 1: Krouse Staging for Inverted Papilloma.
Surgeries were performed under general anesthesia, using an endonasal approach with 0° and 30° endoscopes. A nasal corridor was created by resecting the middle turbinate in some patients, and anterior and posterior ethmoidectomies with unilateral maxillary antrostomy were performed, choosing the most affected nasal cavity by the tumor. Next, a posterior septectomy was done to expose the entire sphenoid from one nasal fossa. The sphenoidotomy was wide. The IP was then resected, starting from the center to induce a central collapse, followed by excision of the lateral remnants in contact with the carotid artery and optic nerve. Bipolar cautery was used for hemostasis. In these cases, the sphenoid was not drilled. In patients with sphenoid sinuses with pneumatization of the pterygoid processes and highly developed lateral recesses, the trans-pterygoid endonasal approach was combined with bilateral sphenoidotomy. For this approach, the pterygoid base was drilled after dissecting the previously described nasal corridor. In IP with synchronous squamous carcinomas, treatment with cisplatin and intensity-modulated radiation therapy (IMRT) was associated with the biopsy or debulking. Follow-up was performed by nasal endoscopy and MRI.
Results
Six patients were evaluated and treated: five males and one female, with IP mainly located in the sphenoid sinus. Two of them had synchronous squamous carcinomas. The youngest patient was 51 years old, and the oldest was 79 years old, with an average age of 66.16 years. The most frequent presenting symptoms were: nasal obstruction (4/6), unilateral in two, bilateral in one, and unilateral associated with decreased visual acuity in another. Two patients with
B A
synchronous squamous carcinoma had decreased visual acuity. One patient was asymptomatic, and the tumor was detected as an incidental finding on imaging.
Imaging showed erosion of the anterior wall of the sphenoid sinus in all patients. The lateral wall was eroded in one, and the floor of the sella turcica was involved in two, one of them associated with erosion of the clivus. The two patients with synchronous carcinomas had intracranial extension of the tumor. No hyperostosis suggesting a site of implantation was detected in the CT scans of any of the patients.
In the four patients with inverted papillomas, an endonasal approach was performed with endoscopes. One patient had a small recurrence at the floor of the sella turcica one year after surgery. He was reoperated and no recurrence was detected during three years follow up. Another patient, 40 days after surgery, began experiencing severe fronto- orbital headache on the left side. The MRI did not show recurrence of the IP.
A month later, he developed left-sided blindness and ptosis (contralateral to the eroded sphenoid lateral wall), and a new MRI revealed infiltration of the right cavernous sinus.
A review of the surgical pathology did not show atypia. Due to the irresectability of the lesion, radiation therapy was initiated. The patient died during radiation therapy from a stroke (Figure1).
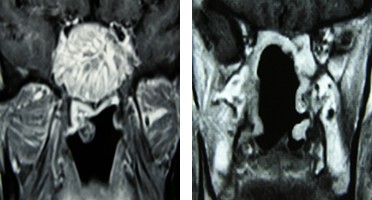
$$ \downarrow $$ Figure 1: Magnetic resonance coronal sections. A: inverted papilloma of sphenoid sinus. B: 45 days postoperatively, a tumor infiltrating the left cavernous sinus is observed (red arrow).
In one patient, subtotal resection was performed as the intraoperative biopsy was reported as inflammatory tissue. After the final diagnosis of inverted papilloma, the patient refused further surgery. A woman who underwent the trans- pterygoid approach had no recurrences during a follow-up of 19 months (Figure 2).

B C
A
D E
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} + \frac {1}{2} \mathrm {C} ^ {2} $$ sphenoid sinus maxillary an- trostomy rinopharynx F G H $$ \downarrow $$
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
procident carotid artery I J K
L M
$$ \swarrow $$
$$ \downarrow $$ Inverted papilloma
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
optic nerve carotid artery $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} + \frac {1}{2} \mathrm {C} ^ {2} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ bony septum in- serted in to carotid artery
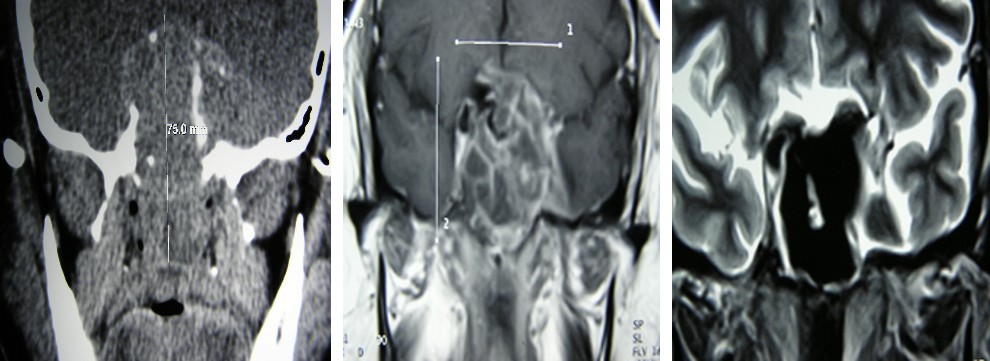
Computed Tomography
A: coronal section. B,C: axial section, where the lateral pneumatization of the sphenoid sinus (yellow arrow) and the prominence of the internal carotid artery with the insertion of a bony septum (red arrow) can be observed.
Magnetic Resonance Imaging
D,E: coronal and axial section where the implantation of the tumor is seen in the paraclival carotid artery (red arrow).
Endoscopic Endonasal Surgical Technique
A: nasal corridor where the maxillary antrostomy bilateral sphenoidotomy with posterior septectomy, and middle turbinectomy are observed.
B: drilling of the pterygoid process to expose the lateral recess of the sphenoid sinus. H,I: the IP is seen in the lateral sphenoid recess. J: carotid artery prominent. K: the sphenoid sinus is seen after complete resection of the IP. L: Posoperative magnetic resonance imaging, coronal section. M: axial section no recurrence of IP is observed in the sphenoid sinus. The two patients who had synchronous squamous cell carcinomas with IP were treated with biopsy/debulking and intensity modulated radiotherapy and concurrent chemotherapy. One of the patients with synchronous squamous carcinoma died with local disease after treatment. The other had no recurrence during a 5-year follow-up (Figure 3).
MRI-A,B: tumor is seen invading the endocranium, involving the optic chiasma and extending to the lateral wall of the nasopharynx. C: MRI showing the disappearance of the tumor after treatment with chemotherapy/radiotherapy In three patients, local control of the disease was achieved; two died, and one had subtotal resection and refused further surgery (Table 2).
| Sex | Age | Symptoms | Images | Surgical Approaches | Pathology | Local Control | |
|---|---|---|---|---|---|---|---|
| M | 77 | unilateral nasal obstruction | lateral wall bone erosion | bilateral sphenoidotomy with posterior septectomy | inverted papilloma | died at 4 months | |
| M | 72 | bilateral nasal obstruction | bone erosion of the clivus and selar region | bilateral sphenoidotomy with posterior septectomy | papilloma invertido con displasia | 3 years without recurrence | |
| M | 79 | asymptomatic (finding in images) | bone erosion of the selar region | subtotal resection (he did not want surgery after the deferred histological diagnosis of PI) | inverted papilloma | ||
| F | 54 | unilateral nasal obstruction | pterygoid pneumatization | transpterigoideo/esfenoidotomia bilateral con septectomia posterior transpterygoid/ bilateral sphenoidotomy with posterior septectomy | inverted papilloma |
Table 2: Patients with inverted papillomas located in the sphenoid sinus.
- bilateral decreased visual acuity
- (optic chiasm involvement) intracraneal extension biopsy / endonasal debulking +
- QT/Rt
- M
- 51 unilateral nasal obstruction/ decreased visual acuity intracraneal extension endonasal biopsy+ Qt/Rt
- M
- 64
Table 3: Patients with inverted papillomas located in the sphenoid sinus.
Discussion
Inverted papilloma located in the sphenoid sinus is rare. One study reported that 12.7% of inverted papillomas treated were located in the sphenoid sinus [2], while another study involving 160 patients treated for inverted papillomas found that 148 (93%) originated in the lateral wall of the nasal cavities and the middle meatus, 5(3%) affected the nasal septum, 3(2%) were in the maxillary sinus, 3(2%) in the sphenoid sinus, and 1(1%) in the frontal sinus [3]. In our personal series of 51 treated inverted papillomas, we had 6 cases with sphenoidal localization, four inverted papillomas, and 2 synchronous squamous carcinomas with inverted papillomas (11.7%). In a literature review, Guillemaud and collaborators found that the most common presenting symptoms of inverted papillomas with sphenoidal localization were: headache (52.1%), nasal obstruction (43.8%), and epistaxis (22.9%) [2], in our cases, the most frequent symptom was nasal obstruction in 4 patients, followed by visual acuity changes (in patients with inverted papilloma and synchronous carcinoma). CT imaging diagnoses sphenoid sinus occupancy and the presence of bone erosion, which can occur in the absence of malignancy. It can also reveal areas of hyperostosis in the form of plaques, which some associate with the implantation site of the inverted papilloma [4]. In our series, the incidence of bone erosion was high. It was diagnosed in three of the four inverted papilloma cases and in two with synchronous carcinoma, who also had intracranial extension. We did not detect areas of hyperostosis.
The treatment for inverted papilloma located in the sphenoid sinus is complete surgical resection. Endonasal approaches with video-endoscopes facilitate inverted papilloma excision as they allow for proper visualization with magnification and angles. Several studies demonstrate a lower recurrence rate for IP treated with endonasal surgery compared to open techniques [5, 6]. Some authors suggest that a key point in surgery is the identification, through imaging or intraoperatively, of areas of hyperostosis that may indicate the implantation site of the inverted papilloma, to be more aggressive in that sector by drilling the underlying bone [7, 8]. Resection or drilling of the bone is recommended by some to remove microscopic tumor remnants that might persist between bony prominences [9]. While this is useful in the maxillary sinus, it is more difficult in the sphenoid because the bone is thinner, and there may be dehiscences or erosions, increasing the risk of injury to vital structures and causing severe complications.
In our case series, we did not find any area of hyperostosis that could indicate the implantation site.
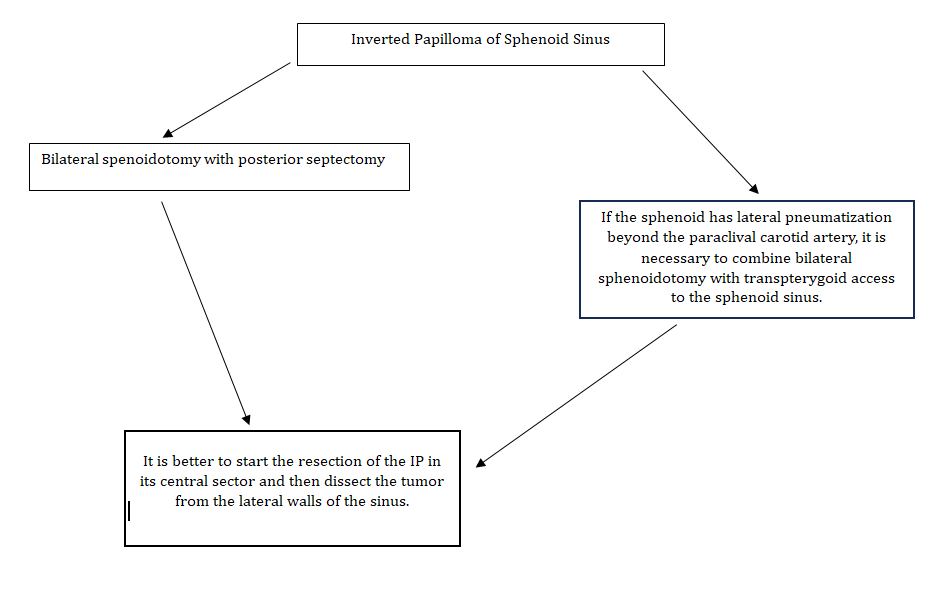
We prefer to use a central resection technique for the inverted papilloma, then dissect and remove the lateral portions of the tumor adjacent to vital structures (Figure 4). Achieving clear margins in inverted papillomas located in the sphenoid sinus is challenging. We believe that intraoperative biopsies to ensure clear margins are of little use, as at the end of the surgery, only bone remains, with no mucosa to assess. It is important to consider the degree of pneumatization of the sphenoid sinus, as sinuses with pneumatization of the pterygoid process often have lateral recesses extending behind the posterior wall of the maxillary sinus, which may hinder exposure via a medial endonasal approach. As Vinciguerra and colleagues suggest [10], a trans-pterygoid approach combined with wide sphenoidotomy should be performed in such cases, as we did in one patient in our series. Also, in cases of excessive pneumatization, the carotid artery or optic nerve may be more prominent or dehiscent and more exposed to injury.
The presence of bone erosion makes complete resection difficult due to the possible extension of the inverted papilloma to areas such as the cavernous sinus or sella turcica. In one of the cases with bone erosion and dehiscence of the paraclival carotid, there was bleeding from the cavernous sinus, which was managed with hemostatic material. One study reported recurrence in 5 out of 7 patients treated surgically for sphenoid inverted papilloma [11]. In a literature review including 48 patients treated with endoscopic surgery between 1996 and 2014, a recurrence rate of 16.66% (8/48) was found [12]. The authors concluded that inverted papillomas implanted in the lateral wall of the sphenoid over the carotid artery or optic nerve, or those with foci of dysplasia or carcinoma in situ, had a higher likelihood of recurrence. In two inverted papillomas in our series, the tumor appeared to originate in the lateral wall over the internal carotid artery, and in another, in the sella turcica. In our study, the recurrence of inverted papillomas was high, but in one patient, the surgery was subtotal as the intraoperative biopsy was reported as inflammatory tissue, and we decided not to resect more tissue over the carotid and the second cranial nerve. With the deferred histopathological diagnosis of inverted papilloma, the patient refused further surgery. Another patient had a recurrence at the level of the sella turcica, was reoperated, and local control of the disease was achieved.
Another patient, who had complete resection of the inverted papilloma confirmed by MRI, had a poor outcome with subsequent invasion of the cavernous sinus and died during radiation treatment. We interpret this aggressive behavior with contralateral cavernous sinus invasion as being due to the existence of an undetected focus of carcinoma, which was not identified in the histopathological examination of the surgical specimen or in the review. The incidence of malignancy in inverted papillomas is variable. A review of 65 case series, including 3181 patients, reported atypia in 88 of 958 (1.1%), dysplasia in 9 of 454 (1.9%), and carcinoma in situ in 15 of 494 (3%). Synchronous carcinomas were diagnosed in 6.8% and metachronous carcinomas in 3.6% [13]. In inverted papillomas of sphenoidal location, dysplasias and carcinomas in situ were found in 6 of 48 patients (12.5%) [2].
Conclusions
Inverted papilloma localized in the sphenoid sinus is rare. The final local control rate we achieved in three patients treated through endonasal approaches with endoscopes for curative purposes was 66.66%. Local control in synchronous carcinomas with inverted papilloma staged as T4-b was 50%. The main endonasal technique is wide paraseptal sphenoidotomy. We prefer to perform a central resection of the tumor and then dissect the lateral walls of the sinus. In cases of extensive pneumatization of the sphenoid and the presence of lateral recesses, we believe it is better to combine sphenoidotomy with a trans-pterygoid approach.
References
-
Krouse JH (2000) Development of a staging system for inverted papilloma. Laryngoscope 110(6): 965-968.
-
Guillemaud JP, Witterick IJ (2009) Inverted Papilloma of the Sphenoid Sinus: Clinical Presentation, Management, and Systematic Review of the Literature. Laryngoscope 119: 2466-2471.
-
Lawson W, Kaufman M, Biller H (2003) Treatment Outcomes in the Management of Inverted Papilloma: An Analysis of 160 Cases. Laryngoscope 113: 1548-1556.
-
Lund VJ, Howard DJ, Wei IW (2014) Tumors of the Nose, Sinuses, and Nasopharynx. Epithelial Epidermoid Tumors, pp: 77-92.
-
Krouse JH (2001) Endoscopic treatment of inverted papilloma: Safety and efficacy. American Journal of Otolaryngology 22(2): 87-99.
-
Busquets JM, Hwang PH (2006) Endoscopic resection of sinonasal inverted papilloma: a meta-analysis. Otolaryngol Head Neck Surg 134: 476-482.
-
Lee DK, Chung SK, Dhong HJ, Kim HY, Kim HJ, et al. (2007) Focal hyperostosis on CT of sinonasal inverted papilloma as a predictor of tumor origin. AJNR Am J Neuroradiol 28(4): 618-621.
-
Zabolotnyi D, Zabolotna D, Zinchenko D, Tsvirinko I, Kizim Y (2020) Diagnosis and Treatment of Patients with Sinonasal Inverted Papilloma. Georgian Med News (306): 31-37.
-
Chiu AG, Jackman AH, Antunes MB, Feldman MD, Palmer JN (2006) Radiographic and Histologic Analysis of the Bone Underlying Inverted Papillomas. Laryngoscope 116: 1617-1620.
-
Vinciguerra A, Guichard JP, Verillaud B, Herman P (2018) Extended sphenoidotomy combined with transpterygoid approach for sphenoidal sinus inverted papilloma. Eur Arch Otorhinolaryngol 280(12): 5369-5378.
-
Cho HJ, Kim JK, Kim K, Kim YS, Lee JG, et al. (2008) Endoscopic surgery for inverted papilloma originating from the sphenoid sinus and related clinical characteristics. Acta Oto-Laryngologica 128: 1120-1125.
-
Suh JD, Ramakrishnan VR, Thompson CF, Bradford A (2015) Inverted Papilloma of the Sphenoid Sinus: Risk Factors for Disease Recurrence. Laryngoscope 125: 544- 548.
-
Lund VJ, Stammberger H, Nicolai P (2010) European position paper on endoscopic management of tumors of the nose, paranasal sinuses and skull base. Rhinol Suppl (22): 1-143.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?