Epidemiology and Etiology of Subjective Tinnitus: A Hospital Study in Chad
Background: Globally, approximately 14.4% of the adult population experiences tinnitus, albeit with variations across continents. In Chad, specific data on this condition is scarce. The objective of this study was to determine the prevalence, socio-professional profile and etiological factors of subjective tinnitus at the Renaissance University Hospital Center in N'Djamena, Chad. Methods: This was a prospective cross-sectional study conducted from January 1st to December 31st, 2022, at the ENT Department of the Renaissance University Hospital Center in N'Djamena. All patients aged 6 years or older who had consulted for subjective tinnitus were included. Results: There was a hospital prevalence of 14.2%. Male-to-female ratio was 2:1. The median age of patients was 40 years. Regarding aetiology, chronic suppurative otitis media accounted for 25.8% of cases, prolonged exposure to noise contributed to 16.7% of cases, acoustic trauma was implicated in 11.7% of cases, presbycusis was identified in 10.0% of cases and drug ototoxicity played a role in 7.5% of cases. Conclusion: Subjective tinnitus is common in our context, especially among young adult males. However, most of the causes are preventable. This study underscores the need to raise awareness about the various aetiological factors associated with tinnitus.
Taoussi AA¹*, Ndoubabé B¹ and Yusra AA²
¹Department of Otolaryngology (ENT)and Head and Neck Surgery, Renaissance University Hospital Center, Chad ²Department of Internal Medicine, Renaissance University Hospital Center, Chad
Abbreviations
ENT: Ear, Nose and Throat; THI: Tinnitus Handicap Inventory; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; SPSS: Statistical Package for the Social Science.
Introduction
Subjective tinnitus is the term used for sounds perceived in the ear without any external auditory stimulus, and they are only heard by the patient [1]. The perceived sounds can manifest in various ways, resembling buzzing, whistling, grinding, ringing, murmuring, humming or chirping. The intensity, frequency and character of these auditory sensations can also vary [2]. While most patients manage these symptoms well, there are instances when they become intrusive, significantly impacting the patient’s quality of life. These effects may include sleep disturbances, attention difficulties, and even anxiety or depression reactions.
Tinnitus affects a substantial portion of the global adult population with an estimated prevalence of 14.4% [3]. However, this prevalence varies across continents. In South America, the prevalence among adults reaches 21.9% [3], In Europe, it is slightly lower at 14.7% [4]. East Asia exhibits a wide range, spanning from 4.3% to 51.3%, all depending on specific studies [5, 6]. Unfortunately, data about tinnitus in Africa remain scarce, with approximately 5% of the population affected [7]. Subjective tinnitus can arise from various factors, including excessive noise exposure, head trauma, hearing disorders, stress and anxiety [8, 9]. Additionally, lifestyle habits, such as smoking and excessive alcohol consumption, may contribute to its development. It’s crucial to recognize that each case of subjective tinnitus is unique, resulting from a combination of those factors. This understanding is essential for effective therapeutic approaches. Tinnitus management involves a multidisciplinary approach, which may include cognitive-behavioural techniques, sound therapies, hearing aids, specific treatments that are tailored into their individual needs.
In developing countries like Chad, data on subjective tinnitus are scarce, hindering the development of effective prevention and management strategies. This study aims to determine the prevalence of subjective tinnitus, and to identify the socio-professional profile and etiological factors of patients at the Renaissance University Hospital Center in N’Djamena. The findings will help improve management and prevention strategies.
Materials and Methods
We conducted a prospective cross-sectional study between January 1st, 2022 to December 31st, 2022 in the Ear, Nose and Throat (ENT) and Cervicofacial Surgery Department, at the Renaissance University Hospital Center in N’Djamena, Chad.
Patients
The study focused on patients who sought consultation for subjective tinnitus. The inclusion criteria included patients aged 6 years and above, seeking consultation for subjective tinnitus. Exclusion criteria encompassed patients under 6 years of age, individuals who had not provided an informed consent, those with objectively pulsatile tinnitus audible through a stethoscope of vascular origin or due to ear muscle contraction.
Procedure
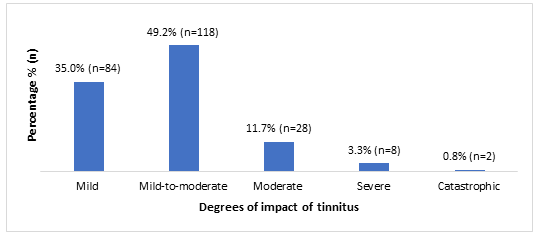
Each patient included in the study underwent a comprehensive evaluation, which included clinical examinations, audiometric tests, and the use of the Tinnitus Handicap Inventory (THI) questionnaire. The THI is a validated tool widely used to measure the impact of tinnitus on patients’ daily lives [10]. Before general implementation, a pre-test of the THI questionnaire was conducted on a small group of patients to ensure its clarity and relevance in our local context. The THI questionnaire, consisting of 25 questions, was then administered in a standardized manner to all patients by a trained healthcare professional. Each question offered three response options: ‘Yes,’ ‘Sometimes,’ or ‘No.’ ‘Yes’ responses were scored four points, ‘Sometimes’ responses two points, and ‘No’ responses zero points. Individual scores were summed to obtain a total score ranging from 0 to 100. This score allows the classification of disabilities into five degrees: mild (0-16), mild-to-moderate (18-36), moderate (38-56), severe (58-76), and catastrophic (78-100).
During the clinical examination, the following elements were taken into account; otoscopy, clinical vestibular examination, assessment of the cranial nerves and auscultation of the neck, mastoauricular region and pre- auricular region. Linear tonal audiometry was performed using an AC50-D® audiometer in a soundproof Puma® Model PRO 25 cabin. The average hearing loss for each ear was calculated by dividing the sum of deficits measured in decibels (dB) at frequencies of 500, 1000, 2000, and 4000 Hz by 4. Deafness was diagnosed when the average hearing loss exceeded 20 dB, in accordance with the classification of the International Bureau of Audiophonology [11]. In the case of an earwax plug, audiometry was performed after the removal of the blockage. For cases of acute middle ear infection accompanied by intense ear pain, audiometry was delayed only if the pain was present and only until the pain subsided, without waiting for the resolution of the conductive component of the hearing loss. In the presence of a conductive or mixed hearing loss with an intact tympanic membrane, impedance audiometry via tympanometry and the study of the stapedial reflexes was performed.
In our study, we systematically prescribed imaging examinations, including CT scans and/or MRIs, for patients presenting with non-pulsatile unilateral tinnitus with asymmetric sensorineural hearing loss. Asymmetric sensorineural hearing loss was defined as a difference of at least 15 dB at two consecutive frequencies, or an average difference of 15 dB or more across the frequencies of 500, 1000, 2000, and 4000 Hz [12]. However, for other cases, imaging was performed based on the diagnostic hypothesis.
Data Collection
We collected data using pre-established forms, capturing essential epidemiological information such as age, gender and profession of the patients. Additionally, we considered relevant medical history, including factors like acoustic trauma, prolonged noise exposure and the use of ototoxic medications. Detailed records were maintained for the tinnitus history, impact assessment scores, and the results of clinical, audiometric and imaging examinations.
Data Analysis
Our data analysis was conducted using SPSS software version 26.0. The results were presented in the form of tables and graphs. The chi-squared test was used to investigate an association between the severity of tinnitus and ototoxic medications. A difference was considered statistically significant if p < 0.05.
Ethical Considerations
We obtained verbal consent from all patients for their participation in the study and the publication of their data. For children aged 6 to 17 years, parental consent was obtained. The study received approval from the Faculty of Human Health Sciences in N’Djamena. We conducted our study in accordance with the ethical principles outlined in the 2013 Helsinki Declaration.
Results
During our study period, 240 patients presented with subjective tinnitus out of a total of 1690 patients that were seen for consultation. This yielded a hospital prevalence of 14.2%. Among these cases, 67.0% (n=160) were male, resulting in a male-to-female ratio of 2:1. The age distribution of the patients ranged from 10 to 85 years, with a median age of 40 years and an average age of 45.3 ± 15.4 years. Notably, children (aged under 18) constituted 2.5% of cases (n=6). Regarding marital status, 81.7% (n=196) of the patients were married. The socio-professional breakdown revealed that unemployed individuals accounted for 35% (n=84) of cases, followed by military personnel at 20% (n=48) and teachers at 13.3% (n=32). For a comprehensive overview, Table 1 provides detailed information on the patients’ socio- professional profile (Table 1).
| n | % | |
|---|---|---|
| Sex | ||
| Male | 160 | 67 |
| Female | 80 | 33 |
| Total | 240 | 100 |
| Age Groups (year) | ||
| [10-30] | 32 | 13 |
| [31-50] | 128 | 53 |
| [51-70] | 64 | 27 |
| [71-90] | 16 | 6.7 |
| Total | 240 | 100 |
| Marital Status | ||
| Married | 196 | 82 |
| Single | 20 | 8.3 |
| Widowed | 20 | 8.3 |
| Divorced | 4 | 1.7 |
| Total | 240 | 100 |
| Occupation | ||
| Unemployed | 84 | 35 |
| Military | 48 | 20 |
| Teacher | 32 | 13 |
| Information Technology (IT) Professional | 24 | 10 |
| Public Finance Officer | 20 | 8.3 |
| Healthcare Personnel | 16 | 6.7 |
| Civil Engineer | 16 | 6.7 |
| Total | 240 | 100 |
Table 1: Socio-professional profile of patients with subjective tinnitus.
In this study, we observed that 50.8% (n=122) of the cases presented with unilateral tinnitus. Also, when considering the duration of symptoms, 60.4% (n=145) had experienced acute tinnitus. Among these patients, 45.4% (n=109) reported that their tinnitus had occurred spontaneously.
However, the auditory sensations varied among the patients, which are 28.3% (n=68) buzzing, 27.5% (n=66) whistling and 20.4% (n=49) ringing. Moreover, 50.4% (n=121) exhibited persistent tinnitus. All these characteristics are summarized in (Table 2).
| n | % | |
|---|---|---|
| Affected Ear Side | ||
| Unilateral (right) | 69 | 29 |
| Unilateral (left) | 53 | 22 |
| Bilateral | 118 | 49 |
| Total | 240 | 100 |
| Duration of Evolution | ||
| Acute (≤6 months) | 145 | 60 |
| Chronic (>6 months) | 95 | 40 |
| Total | 240 | 100 |
| Occurrence Circumstances | ||
| Spontaneous | 109 | 45 |
| Ear infection | 67 | 28 |
| Noise trauma | 40 | 17 |
| Post-medication | 18 | 7.5 |
| Stress or psychological shock | 6 | 2.5 |
| Total | 240 | 100 |
| Characteristics | ||
| Buzzing | 68 | 28 |
| Whistling | 66 | 28 |
| Ringing | 49 | 20 |
| Whispering | 46 | 19 |
| Clicking | 11 | 4.6 |
| Total | 240 | 100 |
| Evolution Mode | ||
| Permanent | 121 | 50 |
| Intermittent | 119 | 50 |
| Total | 240 | 100 |
Table 2: Characteristics of subjective tinnitus in patients.
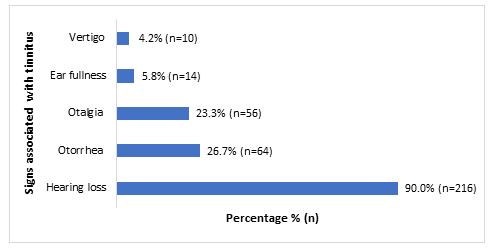
In assessing the impact of tinnitus in patients, 49.2% (n=118) reported that their tinnitus was masked by environmental sounds and easily forgotten during their daily activities. Conversely, 4.2% (n=10) of the patients suffered from debilitating tinnitus, which is characterized as severe and catastrophic. Figure 1 illustrates the distribution of patients based on the tinnitus impact assessment scale. In 90% (n=216) of the cases, tinnitus was associated with hearing loss. Additionally, other related signs are succinctly presented in (Figure 2).
Among the patients, medical histories were primarily associated with 22.9% (n=55) noise exposure, 12.9% (n=31) acute otitis media, 5.8% (n=14) chronic otitis media, 3.3% (n=8) psychological trauma and 2.5% (n=6) hypertension. For a comprehensive overview of the patients’ complete medical and surgical history, refer to (Table 3).
Among the patients, 61.7% (n=148) had a normal otoscopic examination. Pure-tone audiometry revealed that 49.2% (n=118) of patients suffered from sensorineural hearing loss, 27.9% (n=67) had conductive hearing loss, while 12.9% (n=31) exhibited mixed hearing loss. Detailed information is available in (Table 4).
| n | Percentage (%) | |
|---|---|---|
| None | 101 | 42.1 |
| Ear, Nose, and Throat (ENT) | ||
| Acute middle ear infection | 31 | 12.9 |
| Chronic middle ear infection | 14 | 5.8 |
| Rhinitis | 3 | 1.3 |
| Tympanoplasty | 2 | 0.8 |
| Medical | ||
| Noise exposure | 55 | 22.9 |
| Psychological shock | 8 | 3.3 |
| High blood pressure (hypertension) | 6 | 2.5 |
| Malaria | 6 | 2.5 |
| Chronic kidney failure | 4 | 1.7 |
| Migraine | 4 | 1.7 |
| Diabetes | 3 | 1.3 |
| Urinary tract infection | 3 | 1.3 |
| Total | 240 | 100 |
Table 3: Distribution based on the medical-surgical history of patients with subjective tinnitus.
| n | Percentage (%) | |
|---|---|---|
| Otoscopy | ||
| Normal | 148 | 61.7 |
| Pathological* | 92 | 38.3 |
| Total | 240 | 100 |
| Pure-tone audiometry | ||
| Sensorineural hearing loss | 118 | 49.2 |
| Conductive hearing loss | 67 | 27.9 |
| Mixed hearing loss | 31 | 12.9 |
| Normal hearing | 24 | 10 |
| Total | 240 | 100 |
Table 4: Otoscopy and audiology results.
* Pathological otoscopy: An examination that has allowed the identification of various abnormalities affecting the external auditory canal, the tympanic membrane, and the middle ear. Table 4: Otoscopy and audiology results.
In terms of etiology, chronic suppurative otitis media was observed in 25.8% (n=62) of patients, 16.7% (n=40) were exposed to prolonged noise, acoustic trauma was present in 11.7% (n=28) and 10.0% (n=24) exhibited presbycusis. Additionally, 7.5% (n=18) of the patients were affected by drug-induced ototoxicity. Table 5 provides a detailed overview of the causes of subjective tinnitus, while Table 6 and Table 7 illustrate the distribution of causes based on the duration of evolution and the assessment scale for the impact of tinnitus. Notably, there was a statistically significant association (χ²=21.1516; p<0.0001) between medication-induced ototoxicity and disabling tinnitus, as indicated in (Table 8).
| n | Percentage (%) | |
|---|---|---|
| No identified etiology | 26 | 10.8 |
| External ear | ||
| Earwax plug | 10 | 4.2 |
| Middle ear | ||
| Chronic suppurative otitis media | 62 | 25.8 |
| Seromucous otitis media | 6 | 2.5 |
| Sequelae of tympanic perforation | 6 | 2.5 |
| Acute otitis media | 4 | 1.7 |
| Chronic cholesteatomatous otitis media | 4 | 1.7 |
| Otospongiosis | 4 | 1.7 |
| Inner ear and nervous centers | ||
| Chronic noise exposure | 40 | 16.7 |
| Acoustic trauma | 28 | 11.7 |
| Presbycusis | 24 | 10 |
| Ototoxic drug* | 18 | 7.5 |
| Meniere’s disease | 8 | 3.3 |
| Total | 240 | 100 |
Table 5: Distribution of the etiologies of subjective tinnitus.
*Quinine (n=6); furosemide (n=4); gentamicin (n=3); vancomycin (n=3); carbamazepine (n=2). Table 5: Distribution of the etiologies of subjective tinnitus.
| n | |||
|---|---|---|---|
| Etiologies / Duration of evolution | Acute tinnitus | Chronic tinnitus | Total |
| No identified etiology | 16 | 10 | 26 |
| External ear | |||
| Earwax plug | 10 | 0 | 10 |
| Middle ear | |||
| Chronic suppurative otitis media | 28 | 34 | 62 |
| Seromucous otitis media | 5 | 1 | 6 |
| Sequelae of tympanic perforation | 3 | 3 | 6 |
| Acute otitis media | 4 | 0 | 4 |
| Chronic cholesteatomatous otitis media | 1 | 3 | 4 |
| Otospongiosis | 2 | 2 | 4 |
| Inner ear and nervous centers | |||
| Chronic noise exposure | 18 | 22 | 40 |
| Acoustic trauma | 28 | 0 | 28 |
| Presbycusis | 11 | 13 | 24 |
| Ototoxic drug | 14 | 4 | 18 |
| Meniere’s disease | 5 | 3 | 8 |
| Total | 145 | 95 | 240 |
Table 6: Distribution of etiologies based on the duration of subjective tinnitus.
| Mild (0-16) | Mild-to- moderate (18-36) | Moderate (38-56) | Severe | Catastrophic | ||
|---|---|---|---|---|---|---|
| Etiologies / Tinnitus Handicap Inventory (THI) score | (58-76) | (78-100) | Total | |||
| No identified etiology | 13 | 10 | 2 | 1 | 0 | 26 |
| External ear | ||||||
| Earwax plug | 6 | 4 | 0 | 0 | 0 | 10 |
| Middle ear | ||||||
| Chronic suppurative otitis media | 30 | 29 | 3 | 0 | 0 | 62 |
| Seromucous otitis media | 1 | 4 | 1 | 0 | 0 | 6 |
| Sequelae of tympanic perforation | 2 | 3 | 1 | 0 | 0 | 6 |
| Acute otitis media | 1 | 2 | 1 | 0 | 0 | 4 |
| Chronic cholesteatomatous otitis media | 1 | 1 | 1 | 1 | 0 | 4 |
| Otospongiosis | 0 | 2 | 1 | 1 | 0 | 4 |
| Inner ear and nervous centers | ||||||
| Chronic noise exposure | 15 | 23 | 2 | 0 | 0 | 40 |
| Acoustic trauma | 5 | 18 | 4 | 1 | 0 | 28 |
| Presbycusis | 4 | 14 | 6 | 0 | 0 | 24 |
| Ototoxic drug | 4 | 5 | 4 | 3 | 2 | 18 |
| Meniere’s disease | 2 | 3 | 2 | 1 | 0 | 8 |
| Total | 84 | 118 | 28 | 8 | 2 | 240 |
Table 7: Distribution of etiologies based on the scale for assessing the impact of tinnitus.
| Severe to catastrophic disability | Mild to moderate disability | Total | |
|---|---|---|---|
| Ototoxic drugs | 5 | 13 | 18 |
| Other causes | 5 | 217 | 222 |
| Total | 10 | 230 | 240 |
Table 8: Association between drug-induced ototoxicity and disabling tinnitus.
Discussion
In our study, we discovered that 14.2% of the patients seen during hospital consultations exhibited subjective tinnitus. This prevalence aligns closely with global estimates [3], Similarly, European studies have reported comparable rates, albeit with some variations based on specific countries and populations [3, 4], Notably, the prevalence of tinnitus in the United States is approximately 15% [13]. However, it’s essential to highlight that our observed prevalence surpasses that found in prior African studies. For instance, in Egypt, the prevalence is 5.2%, while Guinea reported 5.5%, Togo 2.7% and Nigeria 6.1% [7, 14, 15, 16]. Moreover, our study identified a 4.2% prevalence of disabling tinnitus. Across diverse studies, the rates of disabling tinnitus exhibits considerable variability, ranging from 0.01% to 15.2% [4, 7, 15, 16]. Globally, severe tinnitus affects approximately 2.3% of the population [3], These disparities in the prevalence of tinnitus can be attributed to a combination of factors including the different types, etiology, cultural influences, access to healthcare and research methodologies.
Our study underscores a higher prevalence of tinnitus in men. While some researchers have observed similar trends [16], others have noted a female predominance [4, 6], However, it is essential to recognize that not all studies reveal significant gender-based differences in the prevalence of tinnitus [3, 7], Cultural and social factors play a crucial role in shaping individuals’ perceptions of tinnitus. These factors may influence men and women differently when seeking medical assistance.
The average age of patients in our series was 45.3 years, with a median age of 40 years. Interestingly, these figures align with the typical age at which subjective tinnitus manifests in sub-Saharan Africa [15, 16], Various factors, including noise exposure, infections and underlying medical conditions contribute to the development of tinnitus. While our patient histories correlate with these factors, it is essential to recognize that tinnitus can affect all age groups but its prevalence tends to increase with age [3, 4, 5, 7], Age- related factors, such as hearing loss, may also contribute to this trend.
Regarding the patients’ professions, the results of this study revealed that 35% were unemployed, 20% in the military and 13.3% were teachers. Professions varied across different studies. In the study conducted by Adegbenro et al. in Nigeria, farmers and artisans were predominant [16], In Togo, Foma et al.’s study highlighted a strong presence of traders and homemakers [15]. In South Korea, Kim et al.’s study mainly involved military personnel [6], These diverse professions raise intriguing questions about the relationship between unemployment and tinnitus, as well as the impact of specific noise-exposed occupations. Authors have established a connection between unemployment and tinnitus [17]. Stress factors, financial insecurity and anxiety associated with joblessness may contribute to this correlation. Furthermore, high-risk professions, such as military personnel, get increased exposure to high sound levels due to heavy weapons [6], Workplace noise, whether it’s the chatter in classrooms, the hustle and bustle at a market, or the noise from agricultural machinery, could also increase the risk of tinnitus. In summary, understanding the interplay between professions and tinnitus prevalence is crucial for effective prevention and management strategies.
In our study, 90% of the patients exhibited hearing loss, which was aligning with existing literature. Notably, multiple authors have established a strong correlation between tinnitus and hearing impairment [18, 19], In this study, subjective tinnitus primarily resulted from several causes, ranked in descending order of prevalence; chronic suppurative otitis media (25.8%), prolonged noise exposure (16.7%), acoustic trauma (11.7%), presbycusis (10.0%) and medication-induced ototoxicity (7.5%). These conditions are consistently highlighted in the literature as the common causes of tinnitus [15, 20].
In resource-limited countries like Chad, the convergence of socio-economic constraints (limited access to healthcare), environmental challenges (dust and heat) and health-related issues (insufficient education on ear hygiene) contribute significantly to the elevated incidence of chronic suppurative otitis media. Therefore, consequently experience tinnitus. Subjective tinnitus often results from excessive noise exposure. Whether it’s due to overexposure to loud sounds, acoustic trauma from explosions or deafening concerts, these factors are the primary culprits behind subjective tinnitus. Among soldiers, tinnitus is frequently reported after combat [21].
The link between presbycusis (age-related hearing loss) and tinnitus is evident. As individuals age, the frequency of tinnitus tends to increase. Presbycusis, influenced by factors such as age, genetics, ear diseases, and repeated exposure to loud sounds, remains a major risk factor for tinnitus, particularly in regions with aging populations like Europe. It underscores the importance of proactive measures to safeguard our hearing health.
In our study, several medications have been identified as potential culprits behind tinnitus. These drugs, such as quinine, furosemide, gentamicin, vancomycin and carbamazepine have been extensively documented in scientific literature [13], The study findings reveal a clear association between the severity of tinnitus and ototoxicity. Ototoxicity refers to the harmful effects of certain drugs on the auditory and vestibular systems. Unfortunately, these negative effects are often irreversible, significantly impacting the quality of life of affected individuals. Notably, ototoxicity can lead to profound hearing loss and the accompanying tinnitus can be highly disabling. Beyond this study, similar investigations conducted in Nigeria and Togo had also highlighted frequent cases of tinnitus resulting from medication-induced ototoxicity. In Nigeria, researchers led by Kokong et al. identified drugs like chloramphenicol, chloroquine, and gentamicin as contributors to tinnitus [22], Meanwhile, Foma et al. in Togo reported instances of tinnitus associated with kanamycin, quinine, gentamicin, furosemide and erythromycin [15], Regrettably, ototoxicity remains a persistent challenge in developing African countries. Factors contributing to this issue includes irrational prescriptions of ototoxic drugs, widespread self-medication practices and the over-the-counter sale of medications without proper medical supervision, including illegal street sales.
Conclusion
Subjective tinnitus exhibits a significant prevalence at the Renaissance University Hospital Center in N’Djamena, Chad. This condition primarily impacts young adults and males. Among the profession categories, the most affected groups include the unemployed, military personnel and teachers. The primary contributing factors encompasses chronic middle ear infections, adverse effects of noise exposure and ototoxicity.
Heightened awareness regarding causal factors is imperative. Concurrently, improvements in primary healthcare systems are essential. Education about proper ear hygiene plays a pivotal role in preventing ear infections. Furthermore, public awareness campaigns should highlight the risks associated with excessive noise exposure and therefore, prompting the establishment of noise pollution legislation. Medical practitioners must judiciously prescribe ototoxic medications, guided by thorough audiological examinations. Additionally, regulatory authorities should vigilantly oversee medication sales. By implementing these measures, we can safeguard the auditory health of Chadians and enhance the overall management of subjective tinnitus.
Declarations
Acknowledgments
The authors extend their heartfelt gratitude to all the patients who participated in this study. Moreover, they express their appreciation to the administrative authorities of the Renaissance University Hospital Center for their invaluable and multifaceted support.
Disclosure Statement
No conflict of interest.
Availability of Data and Material
The datasets used and/or analysed during this study are available from the corresponding author upon reasonable request.
Funding
The authors did not receive support from any organizations for this study.
References
-
Guillard R, Decobecq F, Fraysse MJ, Favre A, Congedo M, et al. (2023) Validated French translation of the ESIT-SQ standardized tinnitus screening questionnaire. Eur Ann Otorhinolaryngol Head Neck Dis 140(4): 153-157.
-
Shin SH, Byun SW, Kim SJ, Lee HY (2022) Measures of Subjective Tinnitus: What Does Visual Analog Scale Stand for?. J Am Acad Audiol 33(2): 92-97.
-
Jarach CM, Lugo A, Scala M, van den Brandt Piet A, Cederroth CR, et al. (2022) Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta- analysis. JAMA Neurol 79(9): 888-900.
-
Biswas R, Lugo A, Akeroyd MA, Schleed W, Gallus S, et al. (2021) Tinnitus prevalence in Europe: a multi-country cross-sectional population study. Lancet Reg Health Eur 12: 100250.
-
Zhang D, Xu Q, Caimino C, Baguley DM (2021) The prevalence of tinnitus in China: a systematic review of the literature. J Laryngol Otol 135(1): 3-9.
-
Kim HJ, Lee HJ, An SY, Sim S, Park B, et al. (2015) Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS One 10(5): e0127578.
-
Khedr EM, Ahmed MA, Shawky OA, Mohamed ES, El Attar GS (2010) Epidemiological study of chronic tinnitus in Assiut, Egypt. Neuroepidemiology 35(1): 45-52.
-
Ralli M, Balla MP, Greco A, Altissimi G, Ricci P (2017) Work-Related Noise Exposure in a Cohort of Patients with Chronic Tinnitus: Analysis of Demographic and Audiological Characteristics. Int J Environ Res Public Health 14(9): 1035.
-
Wang X, Jin Y, Cui Z, C Yu, J Yang (2023) Research advances in the correlation between chronic subjective tinnitus and anxiety state. J Clin Otorhinolaryngol Head Neck Surg 37(5): 393-398.
-
Newman CW, Jacobson GP, Spitzer JB (1996) Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg 122(2): 143‑148.
-
Bureau International d’Audiophonologie (BIAP) (1996) International Audiometric Classification of Deafness (BIAP Recommendation 02/1).
-
Snow JB, Wackym PA (1994) Ballenger’s Otorhinolaryngology: Head and Neck Surgery. Williams & Wilkins.
-
Dalrymple SN, Lewis SH, Philman S (2021) Tinnitus: Diagnosis and Management. Am Fam Physician 103(11): 663-671.
-
Keita A, Diallo AO, Keita M (2018) Tinnitus: epidemiology, etiologies and management at the ENT-CCF department of the Donka National Hospital. JNNP 001(17): 31-37.
-
Foma W, Amana B, Lawson SLA (2018) Profile of subjective tinnitus in adults in hospitals in Togo. Case of Sylvanus Olympio University Hospital in Lomé, Med Af Noire 65(4): 209-2016.
-
Adegbenro CA, Amusa YB, Ijadunola IKT (2013) Prevalence of Tinnitus among Nigerians. J Community Med Health Educ 3: 200.
-
Mahboubi H, Oliaei S, Kiumehr S, Dwabe S, Djalilian HR (2013) The prevalence and characteristics of tinnitus in the youth population of the United States. Laryngoscope 123(8): 2001-2008.
-
Shapiro SB, Noij KS, Naples JG, Samy RN (2021) Hearing Loss and Tinnitus. Med Clin North Am 105(5): 799-811.
-
Haider HF, Bojić T, Ribeiro SF, J Paço, DA Hall, et al. (2018) Pathophysiology of Subjective Tinnitus: Triggers and Maintenance. Front Neurosci 12: 866.
-
Samarei R, Fatholahi N (2014) Causes of tinnitus in patients referred to ENT clinic of Imam Khomeini hospital in Urmia, 2012-2013. Glob J Health Sci 6(7): 136-143.
-
Shore SE, Wu C (2019) Mechanisms of Noise-Induced Tinnitus: Insights from Cellular Studies. Neuron 103(1): 8-20.
-
Kokong DD, Bakari A, Ahmad BM (2014) Ototoxicity in Nigeria: why it persists. Ear Nose Throat J 93(7): 256- 264.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?