Mycobacterium Tuberculosis, Culturing and PCR Optimization
The genus Acinetobacter baumannii has undergone substantial taxonomic modifications over the last 30 years. Acinetobacter baumannii is one of the most important representatives of the genus and pathogen for healthcare facilities globally. Over the last 15 years, its clinical significance shows that it has the ability to acquire resistance against antibiotics in this threatening antibiotic era. Naturally A.baumannii can easily be isolated from different sources throughout whole world, found mostly in water, soil, sputum and many healthcare environments, is a non-fermenting, non-spore forming and gram negative coccobacilli. Pneumonia caused by MDR strains of Acinetobacter baumannii creating serious issues for Physicians to treat it properly. Risk factor for two types of patients recognized to pneumonia infection Acinetobacter baumannii hospital associated pneumonia (AHAP) and Acinetobacter baumannii ventilator associated pneumonia (AVAP), by univariate analysis prior to ceftazidime treatment. It is to be reported that potential risk factors for AVAP includes, imipenem resistance, long duration of hospital stay and fluoroquinolones exposure.
Introduction
According to physicians, the most common and severe infections are respiratory tract infections (RTIs) [1]. It has been revealed that risk of RTIs goes to decline with increasing age, incidence of RTIs increases at certain stage of age and subject group i.e. smoking, alcoholism, athletes, chronic and immunosuppressant patients [2]. There are two forms of RTIs, lower respiratory tract infection (LRTI) and upper respiratory tract infection (URTI). About more than 1.5 million deaths, included 24% URTIs and 42% LRTIs are recorded globally from developing countries. In developing countries due to lack of facilities (to eliminate causative agents of RTIs), these countries are facing such problems. There are some environmental impacts also that cause RTIs like outdoor and indoor air pollution, smoke, factory spills and dust etc. upper and lower RTIs about 42% and 20% accounts due to environmental conditions respectively [3]. It has been reported that in United States, Microbial causative agents for RTIs include Acinetobacter baumannii, Pseudomonas aeruginosa, Streptococcus pneumonia, staphylococcus aureus, Haemophillus influenza, Moraxella catarrhalis and Mycobacterium tuberculosis. LRTIs along with Influenza became cause of several deaths [1].
Acinetobacter baumannii Isolation and Significance
The genus Acinetobacter baumannii has undergone substantial taxonomic modifications over the last 30 years. Acinetobacter baumannii is one of the most important representatives of the genus and pathogen for healthcare facilities globally. Over the last 15 years, its clinical significance shows that it has the ability to acquire resistance against antibiotics in this threatening antibiotic era Peleg AY, et al. [4] Naturally A. baumannii can easily be isolated from different sources throughout whole world, found mostly in water, soil, sputum and many healthcare environments, is a non-fermenting, non-spore forming and gram negative coccobacilli. However, it might be possible that it shows gram variable results and occasionally be gram positive on initial stain. Its morphology depends upon growth pattern, bacillary appearance during log phase and coccobacillary appearance during stationary phase. These are oxidase negative, helps to distinguish it from other grams negative organisms like Neisseria, Pseudomonas and Moraxella [5].
In humans mostly of intensive care units (ICUs), abundantly present in normal flora of skin and mucous membrane and cause different type of infections included urinary tract infection, upper respiratory tract infections, ventilator-associated pneumonia, meningitis and septicemia. A.baumannii resists environmental as well as chemical stress included UV, disinfectants, detergents and dehydration [6]. This resistance made A.baumannii a nosocomial infection [7]. It can be isolated from various parts of health facilities, bed, furniture, curtains and equipment. It can disseminate in a number of ways but most common way of its dispersion is the hospital staff [8].
Its emergence of global outbreaks is due to increasing rates of resistance i.e. multidrug resistance. These MDR strains are responsible for the worldwide outbreaks of A.baumannii ’infections [7]. Skin and respiratory track are important sites of colonization of Acinetobacter baumannii. We get its isolates easily from the nares, nasal pharynx and tracheostomy sites. The risk of its colonization increases during ICU stays [9]. Recognized patients are at high risk of infection, should improve hygiene environmental conditions and proper medicine prescription especially related to carbapenem antibiotics.
The health care workers should have high quality trainings in all hospitals departments to prevent from further dispersion of Acinetobacter baumannii infections to others [9]. Pneumonia caused by MDR strains of Acinetobacter creating serious issues for Physicians to treat it properly. Risk factor for two types of patients recognized to pneumonia infection Acinetobacter hospital associated pneumonia (AHAP) and Acinetobacter ventilator associated pneumonia (AVAP), by univariate analysis prior to ceftazidime treatment. It is to be reported that potential risk factors for AVAP includes, imipenem resistance, long duration of hospital stay and fluoroquinolones exposure [5].
Co-infection of A.baumannii and M. tb in MDR- TB Patients
Acinetobacter baumannii may isolate from sputum of known cases of MDR TB patients 1-10%, Tuberculosis is a disease caused by Mycobacterium tuberculosis (MTB). These bacteria are pathogenic and belongs to a family Mycobacteriacea [10]. It was first discovered by Robert Koch in 1882. Tuberculosis is a transferable disease that effect on lungs commonly.
Mycobacterium tuberculosis is announced as second leading infectious agent after HIV that cause AIDS. Throughout Europe and North America it was the epidemic disorder in 18th and 19th century. However it is reported that in mid 1980s TB cases began to rise up worldwide and in 1993 WHO declared first time that TB was a global emergency. In 2015 according to a survey about 1.8 million people died and 1.4 million fell ill with TB [11].
Taxonomy of Tuberculosis
The first scientific taxonomy of Mycobacteria began in 1896 by Lehmann and Neumann. It is included recently in the List of Prokaryotic Names with Standing in Nomenclature (LPSN) database [12].
Mycobacterium has 160 distinct species and divided into three major groups, Mycobacterium tuberculosis Complex (MTBC), M. leprae and Non tuberculosis mycobacteria (NTM). These pathogens are highly intracellular of humans and animals cells. The MTBC has human-associated species include M. tuberculosis, M. africanum, and M. canettii. MTBC also has animal pathogenic species for both domestic and wild animals: M. bovis (Cattle), M. caprae (sheep and goat), M. microti (rodents), M. mongi (banded mangooses), M. orygis (members of the Bovidae family) and M. pinnipeddi (seals and sea lions). It is to be noted that animal-associated species may also have potential as zoonotic pathogens and has ability of transmission to humans to cause infections for example milk borne transmission of TB to humans during pre-pasteurization era [13]. Mycobacterium tuberculosis is a rod shaped long bacterium, 2-4 micrometers in length and 0.2-0.5 micrometers in width. It is non-motile and related distantly to Actinomycetes [14]. They have no structures of locomotion like cilia, obligate aerobe hence they are laying on upper well aerated lobes of lungs [15].
Morphology of M. tuberculosis
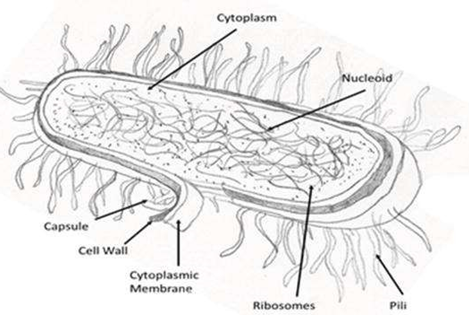
The cell wall of Mycobacterium tuberculosis is of special interest as for the determinant of this bacterium it has virulence characters. The cell wall contains peptidoglycan and 60% lipids and this fraction consists of three major components, mycolic acid, Cord factor and Wax-D [14]. The cell envelop of M.Tb is the causative agent to cause disease, the source of glycoconjugates and other features of the pathogens are involved for it [16] (Figure 1).
The concentration of lipids is so high in Mycobacterium tuberculosis that’s why it attains resistance to many antibiotics, acids and alkaline compounds that are bactericidal. Lipid layer also helps to bacterium to get resistance against lethal oxidation and provide support to get alive in macrophages. Osmotic lysis even in deposition doesn’t occur in this bacterium due to lipid covering. These are impermeable to stains and dyes, once they stain then they don’t de-stain again [14].
The bacterium is a facultative parasite having slow generation time that is 15-20 hours [14], under immunosuppression conditions these bacteria are opportunist pathogens that cause serious infections in human beings. It is to be noted that in vitro microenvironments of hosts are also involve to render M.tb tolerant, involve acidic pH, carbon starvation, nutrient starvation, stationary phase, reactive intermediates of nitrogen, hypoxia, biofilms and streptomycin addicted strain SS18b etc [17].
Culturing of M. tb
There are two types of media used for M. tuberculosis as given:
- Solid media
- Liquid media
- Solid media for its culture includes Lowenstein-Jensen’s media (egg containing), Tarshia medium (Blood agar), Pawlowska medium (potato containing) etc.
- Liquid media for obtaining broth culture of M. tuberculosis includes mostly Middlebrook’s media for obtaining better result within short time duration.
Microscopic Identification of M. tb
Waxy outer covering makes the mycobacterium cell resistant to Gram staining but it sometimes stain Gram positive or Gram negative [18]. For microscopic identification of mycobacterium, stain it with Zeihl-Neelsen (ZN) acid fast stains. This stain has reagents carbol fuchsin (pink dye), acid alcohol, and methylene blue. The smear is fixed and stained with carbol fuchsin after which de stained with acid alcohols. Counterstained the smear with methylene blue to get colored colonies with contrasting background. The bacilli after staining shows as rod like appearance with bright red color. M.tb colonies show small and buff color grown on these media, with some inhibitors also added to remove contaminants during culturing. Within 4-6 weeks colonies are visualized [14].
Review of Literature
Pulmonary tuberculosis is one of the serious respiratory tract infections that frequently cause death worldwide [19]. In 2011 WHO reported 8 million deaths due to tuberculosis worldwide and Pakistan lying at 6th position of the list of the countries globally having high risk of Tb diseased patients. There are the reasons due to which Pakistan get this rank in having Tb cases including transmission and availing resistance to drugs. The pulmonary Tb patients of positive smear acid fast bacilli (AFB) are active patients and playing a role in transmission of the disease through aerosols droplet [20]. People of weak immune systems living in low income regions where TB is endemic and they are in contact with pulmonary TB patients that’s why TB is the 8th leading infectious disease worldwide [21]. Majority of Mycobacterium tuberculosis get resistance to drugs indicating as multidrug resistance (MDR) strains if these strains get resistance to Isoniazid (INH) and Rifampicin (RIF). Both these drugs INH and RIF are given in combination with Ethambutol (EMB) and Streptomycin (STR) [22]. Mycobacterium tuberculosis (M. tb) isolates from TB patients get resistance to certain drugs due to mutations in respective genes and promoter region of genes activating the drug or encoding the drug targets. M. tb develop resistance to RIF due to mutation in rpoB, INH due to resistance in katG and ahpC, EMB get resistance due to change in sequence of embB and pncA [20].
There are following techniques used to identify and diagnose the positive strains of M. tb involving sputum smear microscopy, Gene Xpert MTB/RIF and Culture. Smear microscopy just diagnose the presence of M. tb due to his morphological characteristics but it does not tell about the multi-drug resistance of M. tb strains and hence create hurdles on the treatment of TB patients. To meet the resistance of M.tb, first replace smear microscopy with Gene Xpert MTB/RIF as a baseline diagnostic test in pulmonary TB cases. It has to diagnose the resistance of which drug that M. tb acquire and change the pattern as well drug dosage to treat TB in better way to eliminate the disease, these include Gene Xpert analysis. Gene Xpert MTB/RIF shows the resistance of M.tb against rifampicin [23]. Registered these patients as MDR patients for next follow-ups during treatment to ward off M. tb by using 2nd line antibiotics because they are resistant to 1st line drugs included INH, RIF and EMB. Most of the pulmonary respiratory infected patients are admitted to intensive care units (ICU). As far respiratory tract infection severity to death is concerned the Tb patients that have other respiratory tract infectious agents are more serious cases of concerned. In ICU 60% mortality due to Pulmonary tuberculosis and 25% mortality due to Acinetobacter baumannii hospital associated pneumonia (AHAP) [19].
Lower respiratory tract infection may causes due to almost 8 different microbial strains included Escherichia coli, Acinetobacter baumannii, Klebsiella pneumoniae, Haemophillus influenza, Streptococcus pneumoniae, Pseudomonas aeruginosa, Stenotrophomonas maltophilia and Staphylococcus aureus [24]. Isolate the Acinetobacter baumannii from sputum samples of known cases of MDR-TB patients. For isolation and specify Acinetobacter baumannii, use following media according to laboratory standards like on blood agar showing non hemolytic growth, on Macckonkey agar showing pink to light purple and on Tryptic soy agar show grayish white mucoid appearances after 24- 48 hours incubation at 37 degree Celsius. A.baumannii has oxidase negative, catalase positive and Grams stain negative coccobacilli. To identify Acinetobacter baumannii isolates by molecular characterization (to verify the presence of bla OXA- 51 gene). DNA is isolated by boiling method [25]. Multiplex PCR performed for genotyping of Acinetobacter baumannii isolates to find genes encoding carbapenemases i.e. blaIMP, bla OXA-51-like, bla OXA-23-like, bla OXA-58-like, bla Vim-like, bla -24- like. the PCR process that was performed with initial denaturation at 94℃ for 5 min followed by 33 amplification cycles with denaturation at 94℃ for 25 seconds, annealing at 53℃ for 45 seconds and extension/elongation at 72℃ for 50 seconds followed by final elongation step at 72℃ for 6 minutes. The PCR products include 353bp (bla OXA-51-like), 599bp (bla OXA-
58-like), 501bp (bla OXA- 23-like) and 246bp (bla OXA-24-like) were visualized by horizontal agarose gel electrophoresis stained with Ethidium bromide. The PCR for obtaining the products of metallo beta lactamases encoding blaIMP and blaVIM genes included 30 amplification cycles under following conditions with denaturation at 95℃ for 30 seconds, annealing for 1 minute at specific temperature for each specific gene like annealing temperature for blaVIM is 66℃ and for blaIMP is 45℃, elongation for 1 min at 72℃ and then cycling was followed by final extension at 72℃ for 10 min. The products of 432 bp (i.e. blaIMP) and 500bp were also visualized in agarose gel electrophoresis stained with EtBr [26].
References
-
File TM (2000) The epidemiology of respiratory tract infections. Paper presented at the Seminars in respiratory infections 15(3): 184-194.
-
Jesenak M, Urbancikova I, Banovcin P (2017) Respiratory tract infections and the role of biologically active polysaccharides in their management and prevention. Nutrients 9(7): 779.
-
(2004) Analysis of Estimates of the Environmental Attributable Fraction, by Disease. World Health Organization.
-
Peleg AY, Seifert H, Paterson DL (2008) Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev 21(3): 538-582.
-
Hartzell JD, Kim AS, Kortepeter MG, Moran KA (2007) Acinetobacter baumannii pneumonia: a review. MedGenMed 9(3): 4.
-
Ghajavand H, Esfahani BN, Havaei SA, Moghim S, Fazeli H (2015) Molecular identification of Acinetobacter baumannii isolated from intensive care units and their antimicrobial resistance patterns. Adv Biomed Res 4: 110.
-
Perez F, Hujer AM, Hujer KM, Decker BK, Rather PN, Bonomo RA (2007) Global challenge of multidrug- resistant Acinetobacter baumannii. Antimicrob Agents Chemother 51(10): 3471-3484.
-
Diomedi A (2005) Acinetobacter baumannii pandrug- resistant: update in epidemiological and antimicrobial managing issues. Rev Chilena Infectol 22(4): 298-320.
-
Ardoino I, Zangirolami F, Iemmi D, Lanzoni M, Cargnelutti M, et al. (2016) Risk factors and epidemiology of Acinetobacter baumannii infections in a university hospital in Northern Italy: A case-control study. Am J Infect Control 44(12): 1600-1605.
-
Ryan KJ, Ray CG (2004) Medical microbiology. 4th (Edn.), McGraw Hill 4: 370.
-
McIntosh J (2017) All you need to know about tuberculosis.
-
Lehmann KB, Neumann R (1896) Atlas and ground plan of bacteriology and textbook of special bacteriological diagnostics, 1st (Edn.), Munich.
-
Jagielski T, Minias A, Van Ingen J, Rastogi N, Brzostek A, et al. (2016) Methodological and clinical aspects of the molecular epidemiology of Mycobacterium tuberculosis and other mycobacteria. Clin Microbiol Rev 29(2): 239- 290.
-
Todar K (2015) Textbook of bacteriology.
-
Bennett JE, Dolin R, Blaser MJ (2014) Principles and practice of infectious diseases. 7th (Edn.), Elsevier Health Sciences 1.
-
Angala SK., Belardinelli JM, Huc-Claustre E, Wheat WH, Jackson M (2014) The cell envelope glycoconjugates of Mycobacterium tuberculosis. Crit Rev Biochem Mol Biol 49(5): 361-399.
-
Gold B, Nathan C (2017) Targeting phenotypically tolerant Mycobacterium tuberculosis. Microbiol Spectr 5(1): 10.
-
Fu L, Fu-Liu C (2002) Is Mycobacterium tuberculosis a closer relative to Gram- positive or Gram–negative bacterial pathogens?. Tuberculosis 82(2): 85-90.
-
Erbes R, Oettel K, Raffenberg M, Mauch H, Schmidt- Ioanas M, et al. (2006) Characteristics and outcome of patients with active pulmonary tuberculosis requiring intensive care. European Respiratory Journal 27(6): 1223-1228.
-
Khan SN, Niemann S, Gulfraz M, Qayyum M, Siddiqi S, et al. (2013) Molecular characterization of multidrug- resistant isolates of Mycobacterium tuberculosis from patients in Punjab, Pakistan. Pakistan Journal of Zoology 45(1).
-
Lonnroth K, Castro KG, Chakaya JM, Chauhan LS, Floyd K, et al. (2010) Tuberculosis control and elimination 2010-50: cure, care, and social development. The Lancet 375(9728): 1814-1829.
-
Organization WH, Initiative ST (2010) Treatment of tuberculosis: guidelines: World Health Organization.
-
Daum LT, Peters RP, Fourie PB, Jonkman K, Worthy SA, et al. (2015) Molecular detection of Mycobacterium tuberculosis from sputum transported in PrimeStore® from rural settings. Int J Tuberc Lung Dis 19(5): 552-557.
-
Kang Y, Deng R, Wang C, Deng T, Peng P, et al.(2012) Etiologic diagnosis of lower respiratory tract bacterial infections using sputum samples and quantitative loop- mediated isothermal amplification. PLoS One 7(6): e38743.
-
Babapour E, Haddadi A, Mirnejad R, Angaji SA, Amirmozafari N (2016) Biofilm formation in clinical isolates of nosocomial Acinetobacter baumannii and its relationship with multidrug resistance. Asian Pacific Journal of Tropical Biomedicine 6(6): 528-533.
-
Nanzip NB (2020) Pulmonary Tuberculosis Symptoms, Causes, Pathophysiology, Test, Treatment and Complications.
- Evaluation of Proximate and Mineral Compositions of Momordica charantia L. (Cucurbitaceae)
- Targeting Superbugs: Efficacy of Bacteriophage Therapy against Antibiotic-Resistant Pseudomonas Aeruginosa in Urinary Tract Infections
- Genetic Insights into Prepubertal Gynecomastia: A Comprehensive Analysis of a Rare 45,X[2]/ 46,X, + mar[28] Karyotype
- The Efficiency of Biological Treatment Plants in Some Private Hospitals in the City of Basra, Iraq
- Exploring the Combined Efficacy of Carvacrol and Friedelin against Multi-Drug Resistant Bacteria in Upper and Lower Respiratory Tract Infections
- Isolation, Identification and Comparative Analysis of Oral Microbial Communities in Smokers and Non-Smokers: A Scientific Investigation