Subcutaneous Ureteral Bypass Device for Treatment of Ureteral Obstruction in Persian Breed Female Cat
In the recent years, benign ureteral obstruction by nephrolithiasis has an increased incidence in the feline population, whose causes are not yet fully established. Its diagnosis is based on clinical signs, biochemical analyzes and imaging methods such as radiography and ultrasound. For its treatment, initially one can resort to pharmacological therapy. However, when this is ineffective or contraindicated due to the risk of deterioration of the renal condition, there is a need for surgical intervention. Currently, the subcutaneous ureteral bypass implantation technique is being used more frequently, despite the high cost and periodic mainitance of system functionally. In this case report, we describe the implantation of the subcutaneous ureteral bypass system in a 9-year-old Persian breed female cat with azotemia associated with total obstruction of the right ureter and partial obstruction of the left ureter by nephrolithiasis. In function of total obstruction of right ureter lumen and risk of total obstruction of left ureter lumen was decided by immediate surgery intervention with use of subcutaneous ureteral bypass system. After the implantation of the subcutaneous ureteral bypass system, there was disappearance of azotemia and improvement in the clinical picture and quality life of the cat female.
Introduction
Benign ureteral obstructions in cats have been more frequently described in recent years, can be classified as intraluminal, intramural or extramural, acute or chronic, static or dynamic, unilateral or bilateral and partial or complete [1]. Benign ureteral obstructions in cats are mainly caused by microlithiasis, which may be made up of struvite, calcium oxalate, calcium phosphate, purine, organic debris or have a mixed constitution [2].
In most cases the obstruction is initially unilateral [3]. Inflammation, edema and spasm of the ureter, associated with intraluminal obstruction, lead to aggravation of the obstruction mechanism. Although uncommon, damage from obstruction can lead to rupture of the renal pelvis and ureter, with bleeding and leakage of urine inside abdomen [4, 5].
The formation of uroliths and microlithiasis in cats is not fully established. The causes are believed to involve genetic, infectious, nutritional and environmental factors [6, 7].
The increase in pressure in the renal pelvis and ureter caused by intraluminal obstruction leads to a decrease in renal blood flow to about 40% in the first 24 hours, and later to 20% if total obstruction does not resolve within two weeks. When this ureteral obstruction is chronic, either partial or total, there is an increase in renal blood flow and glomerular filtration rate in the contralateral kidney [8, 9].
Clinical signs associated with ureteral obstruction in cats are nonspecific, and include loss of appetite, weight loss, vomiting, lethargy and altered behavior [8, 10]. Cats with ureteral nephrolithiasis may have azotemia, hyperphosphatemia, hypercalcemia, and hyperkalemia. Normocytic normochromic anemia may be present in 50% of cases of ureterolithiasis and ureteral obstruction in cats [4, 8, 9].
For diagnostic confirmation of ureteral nephrolithiasis, imaging tests such as rx and ultrasonography are indicated. In the x-ray, the lateral view is the most indicated, since the stones are easily identified in the retroperitoneal space. However, the ventrodorsal or dorsoventral projection is important in determining which ureter is involved [8, 11].
Ultrasonography is another important diagnostic method used in cases of suspected ureteral nephrolithiasis, where the visualization of a hyperechoic structure with acoustic shadow and, cranial to it, the presence of a tortuous and dilated ureter and dilated renal pelvis is a typical image of ureteral obstruction. Thus, ultrasonography may be especially useful in determining which ureter is obstructed and assessing the degree of hydroureteronephrosis present [3, 12, 13].
Treatment should be established soon after confirmation of diagnosis as a way of stabilizing the patient, since most animals can have azotemia [14]. Medical therapy is based on promoting diuresis through intravenous fluid therapy, diuretic administration and pain management. Other therapies have been suggested for the relief of pain and displacement of stones along the ureteral lumen, such as the use of amitriptyline and glucagon [14, 15, 16].
However, due to the decrease in renal blood circulation and consequent loss of renal function due to irreversible structural and functional damage, hyperkalemia, overhydration, oliguria/anuria or progressive hydronephrosis, surgical intervention is recommended whenever possible [9, 17]. Among the surgical interventions, the most recent is the implantation of the subcutaneous ureteral bypass system (Figure 1) [1, 2]. This technique is indicated when there is a high risk of re-obstruction [1, 14], ureteral stenosis [18], ureteral stent reaction or intolerance or obstruction secondary to iatrogenic ligament of the ureter during ovariosalpingohysterectomy. It is contraindicated in the presence of coagulopathy or mild hydronephrosis [19].
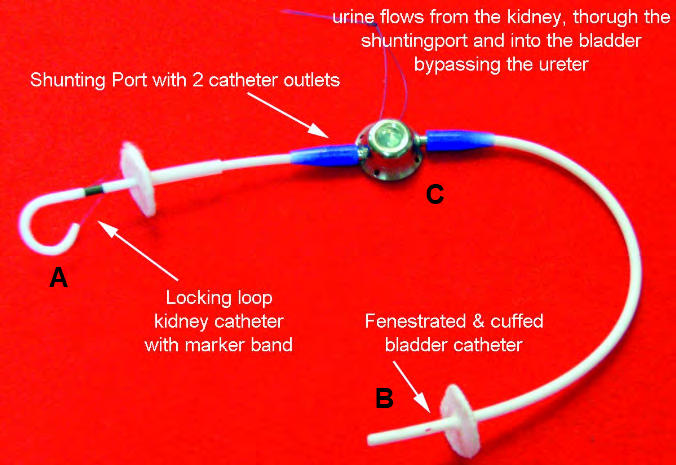
Figure 1: Subcutaneous ureteral bypass system. The system comprising a pigtail catheter with a polyurethane locking loop that is placed in the renal pelvis (A), a radiopaque silicone fenestrated bladder catheter with a polyurethane cuff (B), and a titanium bypass port that is positioned subcutaneously (C). Font: https://veterinary-instrumentation.co.uk/catalog/product/view/id/6787/s/the-sub-a-subcutaneous-ureteral- bypass-system/category/1960/
Case Report
An animal of feline species, female, Persian breed, 9 years old, castrated, vaccinated, without history of previous disease or comorbities, was treated at a private veterinary clinic with a history of inappetence and prostration. Clinical examination showed hyperthermia, dehydration, pale mucous membranes and a full urinary bladder during abdominal palpation.
Complete blood count, biochemical profile and venous blood gas analysis were performed. The blood count showed leukocytosis (32,34 mil/mm3; normal values=5,5-19,5 mil/ mm3). In the evaluation of renal function, azotemia was observed with an increase in serum urea values (68 mg/ dL; normal values=10-56 mg/dL) and creatinine (1,8 mg/ dL; normal values=0,60-1,60 mg/dL). Serum potassium levels were increased (5,9 mmol/L; normal values=3,5-5,1 mmol/L), as well as blood glucose (143 mg/dL; normal values=60-132 mg/dL). In venous blood gas analysis, an increase in PCO2 was observed (53,0 mmHg; normal values=34,0-38,0 mmHg).
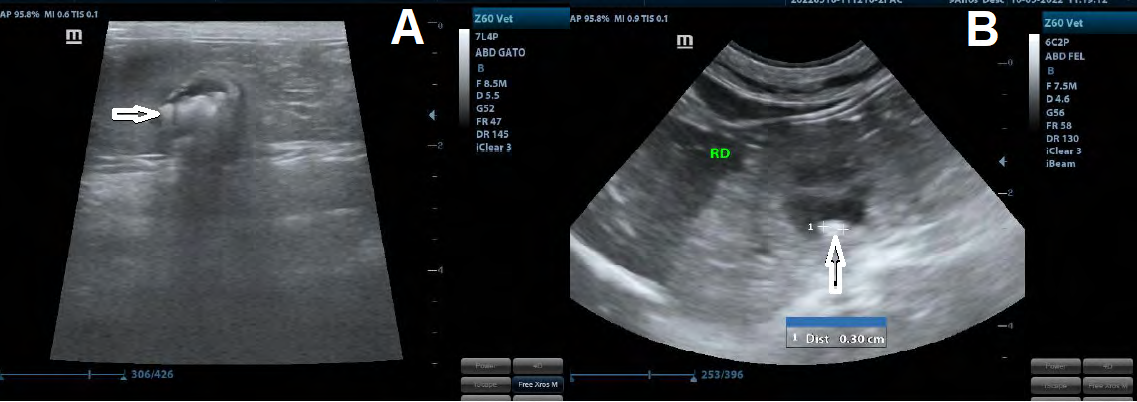
Abdominal ultrasonography was performed, where it was verified that the left kidney measured approximately 3.0 cm and the right kidney 2.98 cm in its major axis. The left kidney showed irregular margins, high echogenicity and loss of corticomedullary architecture and definition, with the presence of several points of mineralization and microlithiasis in the topographic region of pelvic recesses and overlapping the renal pelvis, with a few microlithiasis insinuating themselves into the ureter path (Figure 2A) and intraluminal microlithiasis (0,13-0,21 cm of diameter) in the final third of left ureter (Figure 2B).
The right kidney had irregular margins, high echogenicity and loss of corticomedullary architecture and definition, and dilation of the renal pelvis (hydronephrosis) (Figure 2C). Several points of mineralization and micro stones were observed in the topographic region of pelvic recesses and overlying the renal pelvis. In the right ureter, several intraluminal microlithiasis were observed throughout its path (0,11-0,49 cm of diameter), blocking your lumen (Figure 2D).
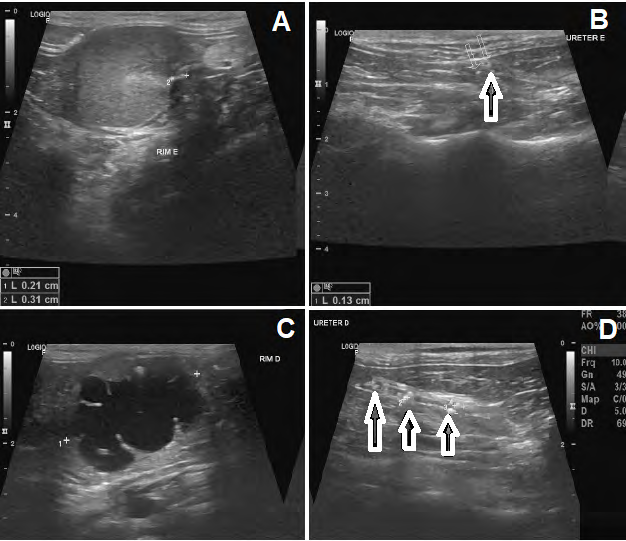
Figure 2: Abdominal ultrasonography of kidneys and ureters. A. Left kidney with irregular margins, high echogenicity and loss of corticomedullary architecture and definition. Mineralization points in pelvic recess. B. Presence of intraluminal microlithiasis (0.13-0.21 cm of diameter) in the final third of the left ureter (arrow). C. Right kidney with irregular margins, high echogenicity and loss of corticomedullary architecture and definition with significant dilation of renal pelvis (hydronephrosis). D. Right ureter with presence of microlithiasis since cranial third to caudal third, measuring between 0.11 to 0.49 cm, causing obstructive process. Font: Errante, 2022.
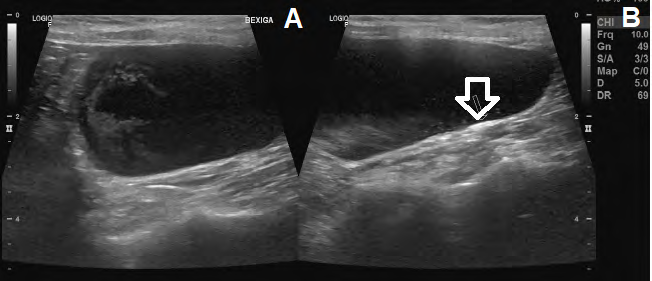
The urinary bladder was distended, containing anechoic content and sediment in suspension (Figure 3A), slim and regular wall (Figure 3B).
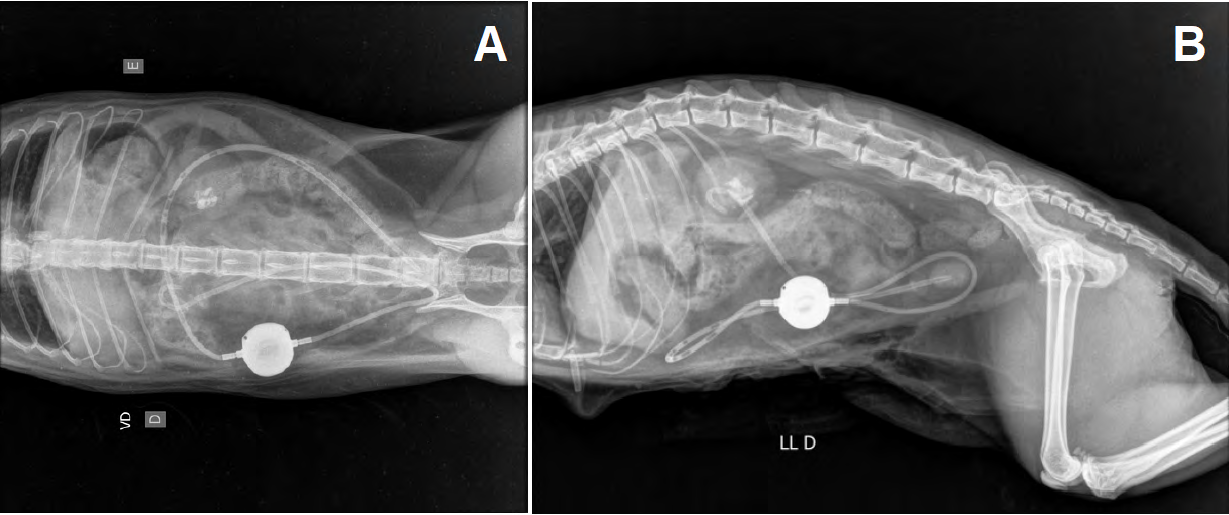
Due to the total obstructive condition of the right ureter without possibility of microlithiasis migration to the bladder and partial obstruction of the left ureter by microlithiasis and azotemia, the tutor was advised to perform a surgical intervention for the implantation of the subcutaneous ureteral bypass system. The system was implemented by a specialist in the field of Veterinary Urology and Nephrology. After the surgery, radiography (Figure 4) and abdominal ultrasonography (Figure 5) were performed to check the implantation of subcutaneous ureteral bypass system.
After implantation of the subcutaneous ureteral bypass system, the cat female was submitted to fluid therapy with the administration of Ringer Lactate (45-74/ml/kg/day intravenous) to correct hydration and promote diuresis. The buprenorphine was used for pain management (0,01/mg/ kg/day intramuscular) during three days, and for infection control the association amoxicillin + potassium clavulanate (20 mg/kg/twice a day/during 14 days, oral route).
After two weeks of treatment, a new complete blood count, biochemical profile and venous blood gas analysis were performed. The number of leukocytes, the serum values of urea, creatinine, potassium and PCO2 returned to normal parameters for the species.
The tutor was instructed to provide a specific diet to prevent the formation of calcium oxalate microlithiasis and by reducing the concentration of calcium and oxalates in the urine, in addition to reducing the acidity of the urine. Was also advised to allow the subcutaneous ureteral bypass system was be flushed every three months to reduce the risk of system obstruction. To the control of urinary infection, realization of urine culture every three months in the first year after surgery, and after this period, urine culture every 6 months.
Discussion
Benign ureteral obstruction in cats can be caused by microlithiasis, ureteral stricture, infection, dry solidified blood, and retroperitoneal fibrosis secondary to iatrogenic ureteral ligation or kidney transplantation [1, 20, 21].
Clinical signs associated with ureteral obstruction in cats are nonspecific, and include loss of appetite, weight loss, vomiting, lethargy, and behavior change [8, 10], clinical signs described by the female cat’s owner in this case report.
Laboratory tests for suspected ureteral microlithiasis in cats include a complete blood count, biochemical profile, and venous blood gas analysis. Findings such as leukocytosis, increased serum urea and creatinine levels [8, 22] and potassium [23, 24] are referred to in the literature and were described in our case report. In the vast majority of cases, cats with benign ureteral obstruction have chronic kidney disease and may have azotemia at the time of clinical symptoms [4, 8].
Imaging tests such as radiography and ultrasonography are important for confirmation of ureteral obstruction and medical/surgical management to be defined [3, 8, 11, 12, 13]. Based on the ultrasonography imaging findings, we can establish the best approach to be used in our case report.
When pharmacological treatment does not improve the clinical and obstructive condition, surgical treatment is indicated, implantation of the subcutaneous ureteral bypass system is a safe and effective option, which leads to immediate decompression of the renal pelvis, decrease in serum urea and creatinine concentration [1, 2], abdominal discomfort and pain [25].
The medical treatment many times is inefficient, leading diminish of creatinine serum levels in only 13% of cats treated [26], and ureteral surgeries can associate with high mortality (until 22%) [17, 26, 27]. The use of ureteral stenting leads to minor mortality (until 9%), but the surgery is very challenged and ureteral recurrent obstruction can be occurred with more frequency [17], with need of stenting change in 27% of cases [28]. In function this, we decided by the use of subcutaneous ureteral bypass device, a security option in the treatment of benign ureteral obstructions in cats and this benefice in terms of rapid decrease of azotemia, clinical recuperation and low percentual of obits and complications after surgery [29, 30, 31, 32].
The use of subcutaneous ureteral bypass device is indicated when there is a high risk of re-obstruction [1, 14], ureteral stenosis [18], ureteral stent reaction or intolerance or obstruction secondary to iatrogenic ligament of the ureter during ovariosalpingohysterectomy. It is contraindicated in the presence of coagulopathy or mild hydronephrosis [19]. In function of total obstructive condition of the right ureter without possibility of microlithiasis migration to the bladder and partial obstruction of the left ureter by microlithiasis, azotemia and absence of comorbities was decide the use of subcutaneous ureteral bypass system in our case report.
Through laboratory and imaging tests after the surgery, we were able to verify the decompression of the renal pelvis and the decrease in serum levels of urea and creatinine facts described by literature [13, 16]. Abdominal discomfort and pain disappear three days after surgery, also aided by pain management with buprenorphine, a fact described by the cat’s owner. After 14 days of fluid therapy and antibiotic therapy, azotemia and leukocytosis disappeared, respectively.
After the surgery of female cat, was recommended a specific diet to prevent the formation of calcium oxalate microlithiasis and by reducing the concentration of calcium and oxalates in the urine, in addition to reducing the acidity of the urine [33, 34].
The implantation of the subcutaneous ureteral bypass device must be performed by trained veterinarians, which led us to turn to a specialist in the field of Veterinary Urology and Nephrology. This surgical treatment option increases survival and quality of life in life-threatening animals at the time of diagnosis [28, 30, 31], as we observed in our case report.
Conclusion
The use of subcutaneous ureteral bypass device is indicated in a high risk of ureteral re-obstruction, ureteral stenosis, ureteral stent reaction or intolerance or obstruction secondary to iatrogenic ligament of the ureter during ovariosalpingohysterectomy. Because the impossibility of complete passage of microlithiasis through the lumen of the right ureter through medical intervention in our case report, risk of total obstruction of left ureter and absence of comorbities, the introduction of subcutaneous ureteral bypass was a surgical option that does not caused relevant damage to the renal parenchyma and ureter, leading to a rapid decrease of azotemia. This surgery not recommended in all situation of ureteral obstruction, such as coagulopathy or mild hydronephrosis. In our case report we check the surgery of subcutaneous ureteral bypass device allowed a significant improvement in the laboratorial results and clinical quality in the life of female cat.
References
-
Wuillemin F, Vachon C, Beauchamp G, Dunn M (2021) Subcutaneous ureteral bypass device placement in 81 cats with benign ureteral obstruction (2013-2018). J Vet Intern Med 35(6): 2778-2786.
-
Berent A, Weisse CW, Bagley DH, Lamb K (2018) Use of a subcutaneous ureteral bypass for treatment of benign ureteral obstruction in cats: 174 ureters in 134 cats (2009-2015). J Am Vet Assoc 253(10): 1309-1327.
-
Lamb CR, Cortelini S, Halfacree Z (2018) Ultrasonography in the diagnosis and management of cats with ureteral obstruction. J Feline Med Surg 20(1): 15-22.
-
Shipov A, Segev G (2013) Ureteral obstruction in dogs and cats. IJVM 68: 71-77.
-
Cockburn E, Battersby IA, Doyle RS (2021) Renal pelvic ruptures, intrapelvic haematoma and retroperitoneal haemorrahage associated with obstructive ureterolithiasis in a cat. J Small Anim Pract 62(7): 599- 603.
-
Adams LG (2013) Nephroliths and ureteroliths: a new stone age. N Z Vet J 61(4): 212-216.
-
Ichii O, Oyamada K, Mizukawa H, Yokoyama N, Namba T, et al. (2022) Ureteral morphology and pathology during urolithiasis in cats. Res Vet Sci 151: 10-20.
-
Kyles AE, Hardie EM, Wooden BG, Adin CA, Stone EA, et al. (2005) Clinical, clinicopathologic, radiographic, and ultrasonographic abnormalities in cats with ureteral calculi: 163 cases (1984-2002). J Am Vet Med Assoc 226(6): 932-936.
-
Clarke DL (2018) Feline ureteral obstructions Part 1: medical management. J Small Anim Pract 59(6): 324- 333.
-
Steinhaus J, Berent AC, Weisse C, Eatroff A, Donovan T, et al. (2015) Clinical presentation and outcome of cats with circumcaval ureters associated with a uretheral obstruction. J Vet Intern Med 29(1): 63-70.
-
Berent AC (2016) Interventional radiology of the urinary tract. Vet Clin North Am Small Anim Pract 46(3): 567- 596.
-
Wormser C, Reetz JA, Drobatz KJ, Aronson LR (2019) Diagnosis utility of ultrasonography for the detection of the cause and location of ureteral obstruction in cats: 71 cases (2010-2016). J Am Vet Med Assoc 254(6): 710- 715.
-
Lemieux C, Vachon C, Beauchamp G, Dunn ME (2021) Minimal renal pelvis dilation in cats diagnosed with benign ureteral obstruction by antegrade pyelography: a retrospective study of 82 cases (2012-2018). J Feline Med Surg 23(10): 892-899.
-
Berent AC (2011) Ureteral obstructions in dogs and cats: a review of traditional and new interventional diagnostic and therapeutic options. J Vet Emerg Crit Care (San Antonio) 21(2): 86-103.
-
Hardie EM, Kyles AE (2004) Management of ureteral obstruction. Vet Clin North Am Small Anim Pract 34(4): 989-1010.
-
Milligan M, Berent AC (2019) Medical and interventional management of upper urinary tract uroliths Vet Clin North Am Small Anim Pract 49(2): 157-174.
-
Wormser C, Clarke DL, Aronson LR (2016) Outcomes of ureteral surgery and ureteral stenting in cats: 117 cases (2006-2014). J Am Vet Med Assoc 248(5): 518-525.
-
Defarges A, Berent A, Dunn M (2013) New alternatives for minimally invasive management of uroliths: ureteroliths. Compend Contin Educ Vet 35(3): E4.
-
Johnson CM, Culp WT, Palm CA, Zacuto AC (2015) Subcutaneous ureteral bypass device for treatment of iatrogenic ureteral ligation in a kitten. J Am Vet Med Assoc 247(8): 924-931.
-
Aronson LR (2002) Retroperitoneal fibrosis as a postoperative complication following renal transplantation in cats. J Feline Med Surg 24(4): 304- 310.
-
Byer BJ, Hardie RJ, McAnulty JF (2022) Retroperitoneal fibrosis as a postoperative complication following renal transplantation in cats. J Feline Med Surg 24(4): 304- 310.
-
Cray M, Berent AC, Weisse CW, Bagley D (2018) Treatment of pyonephrosis with a subcutaneous ureteral bypass device in four cats. J Am Vet Med Assoc 252(6): 744-753.
-
Garcia de Carellan Mateo A, Brodbelt D, Kulendra N, Alibhai H (2015) Retrospective study of the perioperative management and complications of ureteral obstruction in 37 cats. Vet Anaesth Analg 42(6): 570-579.
-
Mauro KD, Bradley CW, Drobatz KJ (2020) Postmortem urinary tract changes in cats with uretheral obstruction J Vet Emerg Crit Care (San Antonio) 30(2): 187-193.
-
Hardie EM, Kyles AE (2004) Management of ureteral obstruction. Vet Clin North Am Small Anim Pract 34(4): 989-1010.
-
Kyles AE, Hardie EM, Wooden BG, Adin CA, Stone EA, et al. (2005) Management and outcome of cats with uretheral calculi: 153 cases (1984-2002). J Am Vet Med Assoc 226(6): 937-944.
-
Culp WT, Palm CA, Hsueh C, Mayhew PD, Hunt GB, et al. (2016) Outcome in cats with benign uretheral obstructions treatment by means of ureteral stenting versus ureterostomy. J Am Vet Med Assoc 249(11): 1292-1300.
-
Berent AC, Weisse C, Bagley D (2014) Technical and clinical outcomes of ureteral stenting in cats with benign ureteral obstructions: 69 cases (2006-2010). J Am Vet Med Assoc 244: 559-576.
-
Livet V, Pillard P, Goy-Thollot I, Maleca D, Cabon Q, et al. (2017) Placement of subcutaneous ureteral bypass without fluoroscopic guidance in cats with ureteral obstruction: 19 cases (2014-2016). J Feline Med Surg 19(10): 1030-1039.
-
Wuilemin F, Vachon C, Beauchamp G, Dunn M (2021) Subcutaneous ureteral bypass device placement in 81 cats with benign ureteral obstruction (2013-2018). J Vet Intern Med 35(6): 2778-2786.
-
Kulendra NJ, Borgeat K, Syme H, Dirrig H, Halfacree Z (2021) Survival and complications in cats treated with subcutaneous ureteral bypass. J Small Anim Pract 62(1): 4-11.
-
Vrijsen E, Devriendt N, Mortier F, Stock E, Van Goethem B, et al. (2021) Complications and survival after subcutaneous ureteral bypass device placement in 24 cats: a retrospective study (2016-2019). J Feline Med Surg 23(8): 759-769.
-
Leckcharoensuk C, Osborne CA, Lulich JP, Osborne CA, Koehler LA, et al. (2001) Association between dietary factors and calcium oxalate and magnesium ammonium phosphate urolithiasis in cats. J Am Vet Med Assoc 219(9): 1228-1237.
-
Bartges JW, Kirk CA, Cox SK, Moyers TD (2013) Influence of acidifying or alkalinizing diets on bone mineral density and urine relative supersaturation with calcium oxalate and struvite in healthy cats. Am J Vet Res 74(10): 1347-1352.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework