Canine Cognitive Dysfunction Syndrome a Challenge in Treatment and Improvement in Quality Life of Older Dogs
The canine cognitive dysfunction syndrome is a chronic and progressive neurodegenerative disease that affects elderly dogs, leading to the emergence of anatomical and functional changes in the central nervous system and development of characteristic behavioral clinical signs, such as memory loss, alteration of the sleep/wake cycle, decreased response to visual and auditory stimuli and hygiene problems that affect the relationship between the animal and the tutor. Although there is no cure for this disease, early diagnosis and installation of treatment are fundamental to improving behavioral clinical signs, quality and increased life expectancy of geriatric dogs.
Introduction
The canine cognitive dysfunction syndrome is a chronic progressive neurodegenerative disease not associated with other conditions such as infections, metabolic disorders or neoplasms. The disease is characterized by behavioral changes, memory loss, hygiene problems, changes in the sleep/wake cycle and in the interaction of dogs with their tutors, being compared to Alzheimer’s disease in humans. The Alzheimer´s disease is a neurocognitive disturbance, being considered the most common cause of dementia in older humans [1, 2].
The clinical signs of canine cognitive dysfunction syndrome are subtle in the early stages and tend to worsen with disease progression [3]. The dogs can get lost in familiar places, try to leave the wrong side of the door, can look fixedly at a location and walk compulsively way. The dogs can also have a change in the sleep cycle/wakefulness, sleeping more during the day and becoming more restless at night, and may cry, vocalize and scratch the floor [1]. The decreased in the locomotor activities and responses to auditory and visual stimuli may occur; dogs may fail to recognize their tutors, may experience confusion, separation anxiety, and aggression, appetite changes and defecating in inappropriate places [3, 4].
The canine cognitive dysfunction syndrome is most common in dogs over the age of 8 years, affecting 14%-35% of the pet dog population [3]. There is no predisposition regarding the breed or size of the dogs, but a higher prevalence of the disease has been described in castrated animals of both sexes. It is believed that estrogen and testosterone may act as neuroprotectants, reducing the accumulation of β-amyloid protein oligomers in neuronal tissue [5, 6].
The pathophysiology of canine cognitive dysfunction syndrome involves ischemic and reperfusion lesions in the brain that produce free radicals of oxygen that cause oxidative damage and increase in monoamine oxidase activity, leading to short-term memory decline, changes in motor function, sleep cycle/wakefulness and anxiety [7].
However, as with Alzheimer’s Disease in humans, the main factor involved in the development of canine cognitive dysfunction syndrome is the alteration in the processing of amyloid precursor protein with the formation and accumulation of β-amyloid protein oligomers (degenerate axons and dendrites, astrocytes and glial cells around an amyloid nucleus). The presence of these β-amyloid protein can alter the activity of kinases and phosphatases leading to hyperphosphorylation of tau (microtubule- stabilizing protein). The deposition of β-amyloid protein in the hippocampus and frontal cortex and in the wall of cerebral blood vessels (cerebral amyloid angiopathy mainly in the occipital cortex) leads to changes in vascular flow, periventricular hypoxia, neuronal degeneration, synaptic dysfunction [8] and depletion of excitatory neurotransmitters such as acetylcholine (involved in memory), dopamine (responsible for motor control), norepinephrine (responsible for warning and attention signals) and serotonin (involved in the control of mood and sleep) [9, 10, 11].
The neuronal compression by deposition of β-amyloid protein in the interstice causes neuronal death and loss of synapses, where the death of noradrenergic neurons causes decline in cognition [7]. The macroscopic structural consequences of all these processes are cerebral atrophy [12], ventricular dilatation and meninges calcification [13]. The decrease in the production of presynaptic and/or postsynaptic transmitters causes impairment of peripheral nervous system with decreased or motors reflexes and muscle atrophy [3, 14].
The early diagnosis provides the installation of immediate treatment, promoting an increase in the quality of life, well-being and longevity of dogs. However, there are no currently specific diagnostic tests for canine cognitive dysfunction syndrome [3, 4]. The diagnosis is realized through a combination of anamnesis, complete physical examination and complementary tests such as blood count, serum biochemistry, urinalysis, echocardiogram, electroencephalography and central nervous system magnetic resonance imaging [3, 12, 15, 16].
The application of specific questions to the owner about the dog’s behavior, sleep/wakefulness status, activity level and orientation, memory, personality changes and disorientation are also important for establishing the diagnosis [3, 15].
Definitive diagnosis can be obtained through magnetic resonance imaging [3, 12] or post-mortem brain study, where is observed macroscopically cortical atrophy and ventricular dilatation. On the histopathological examination, deposition of aggregates of β-amyloid protein (senile plaques) can be found [1]. The use of plasma markers such as β-amyloid protein are under investigation and not used routinely [17].
The differential diagnosis of canine cognitive dysfunction syndrome should include the search for intracranial neoplasms, hepatic encephalopathy, hypothyroidism, cerebrovascular accident, anemia, heart disease and hypertension [18, 19].
Since this disease has no cure, the goals of treatment are to improve the quality of life of dogs and the animal-tutor interaction. This can be achieved through mental and sensory stimulation, pharmacological therapy and nutritional supplementation [3, 20, 21].
Mental and sensory stimulation can be done by removing the furniture where the animal spends most of its time, greater supply in the number of water pots in the place of rest, placement of ramps to facilitate access to certain locations, and use of non-slip material, rugs or carpets in central environments and corridors that facilitate the orientation of the dog through tactile identification [20].
If the dog has problems related to sleep, it should be stimulated during the day with different activities, and at night, kept in a quiet place so that it can sleep. Whenever possible, short walks can be taken gradually in news places to the dogs, stimulating olfactory, auditory and visual exploration [20, 22].
The pharmacological therapy aims to restore neurotransmitter concentrations and should be maintained until the end of the dog’s life [3, 23]. The selegiline is a selective and irreversible inhibitor of monoamine oxidase B that increases levels of dopamine and others neurotransmitter catecholamines in the cortex and hippocampus, promoting improvement of clinical signs of canine cognitive dysfunction syndrome [24].
The pentoxifylline improves brain blood perfusion, has antithrombotic action and improves brain oxygenation, while melatonin can be used in the cases of sleep cycle/ wakefulness disorders [22].
The nicergoline, an antagonist of α-1 and α-2 adrenergic receptors, promotes increased cerebral blood flow and increased production of dopamine and noradrenaline, improving the behavioral state of dogs [25].
The food supplementation with vitamins A, C and E, minerals such as selenium, flavonoids, carotenoids, α-lipoic acid, L-carnitine and omega-3; or the use of diets with high levels of omega-3 and therapeutic levels of L-carnitine are beneficial due to their antioxidant properties [21, 26, 27].
How not have cure for canine cognitive dysfunction syndrome, the tendency is that with the progression of the disease clinical signs will worsen. The impairment of the peripheral nervous system leads to decreased reflexes and muscle atrophy, causing some dogs to stop moving, and may develop complications such as pressure ulcers (Figure 1) and urinary disorders, which are also commonly observed in geriatric dogs [28]. In this way, it is essential educate the tutor about forms of treatment, prognosis and life expectancy of dogs affected [3].
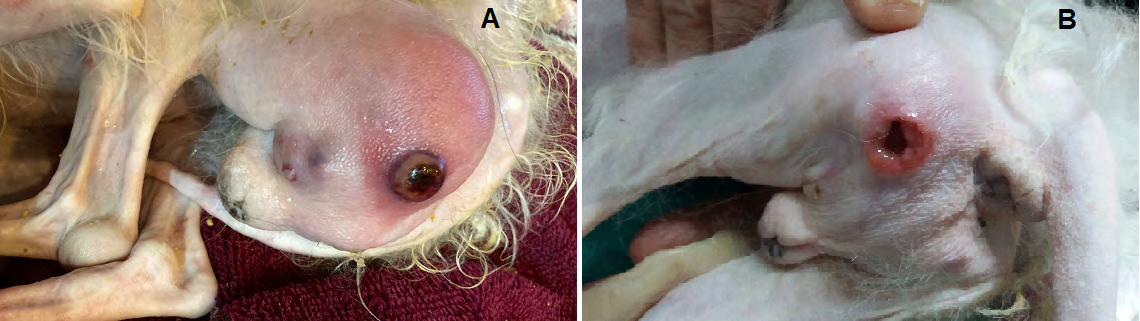
A. Pressure ulcer in function of decreased in motors reflexes and muscle atrophy B. Wound evolution after three days of treatment with hydrocolloid absorbent self-adhesive dressing with calcium alginate. Font: Errante, 2022. Figure 1: Pressure ulcer in a 13-year-old male Poodle breed dog with canine cognitive dysfunction syndrome.
Considerations
The canine cognitive dysfunction syndrome is a chronic neurodegenerative disease that affects older dogs that causes anatomical and functional changes in the central nervous system and that lead to the emergence of characteristic behavioral clinical signs. The early diagnosis allows prompt treatment, delaying the development of clinical signs, that can affect the relationship between dogs with their tutors. The role of the veterinarian is fundamental in orientation of tutors on the need for early installation of different therapy modalities in search of improving the quality and life expectancy of geriatric dogs.
References
-
Prpar Mihevc S, Majdic G (2019) Canine cognitive dysfunction and Alzheimer´s disease-two facets of the same disease?. Front Neurosci 13: 1-18.
-
Pleen J, Townley R (2022) Alzheimer´s disease. J Neurol 269(2): 1038-1051.
-
Dewey CW, Davies ES, Xie H, Waskshlag JJ (2019) Canine cognitive dysfunction: pathophysiology, diagnosis, and treatment. Vet Clin North Am Small Anim Pract 49(3): 477-499.
-
Ozawa M, Inoue M, Uchida K, Chambers JK, Takeuch Y, et al. (2019) Physical signs of canine cognitive dysfunction. J Vet Med Sci 81(12): 1829-1834.
-
Camps T, Amat M, Manteca X (2019) A review of medical conditions and behavioural problems in dogs and cats. Animals (Basel) 9(12): 1133.
-
Habiba U, Ozawa M, Chambers JK, Uchida K, Descallar J, et al. (2021) Neuronal deposition of amyloid- β oligomers and hyperphosphorylated tau is closely connected with cognitive dysfunction in aged dogs. J Alzheimer Dis Rep 5(1): 749-760.
-
Head E, Rofina J, Zicker S (2008) Oxidative stress, aging, and central nervous system disease in the canine model of human brain aging. Vet Clin North Am Small Anim Pract 38(1): 167-178.
-
Urfer SR, Darvas M, Czeibert K, Sandor S, Promislow DEL, et al. (2021) Canine Cognitive Dysfunction (CCD) scores correlate with amyloid beta 42 levels in dog brain tissue. Geroscience 43(5): 2379-2386.
-
Araujo JA, Studzinski CM, Milgram NW (2005) Further evidence for the cholinergic hypothesis of aging and dementia from the canine model of aging. Prog Neuropsypharmacol Biol Psychiatry 29(3): 411-422.
-
Pugliese M, Gangitano C, Ceccariglia S, Carrasco JL, Del Fa A, et al. (2007) Canine cognitive dysfunction and the cerebellum: acetylcholinesterase reduction, neuronal and glial changes. Brain Res 1139: 85-94.
-
Chapagain D, Range F, Huber L, Viranyi Z (2018) Cognitive aging in dogs. Gerontology 64(2): 165-171.
-
Dewey CW, Rishniw M, Johnson PJ, Platt S, Robinson K, et al. (2021) Canine cognitive dysfunction patients have reduced total hippocampal volume compared with aging control dogs: a comparative magnetic resonance imaging study. Open Vet J 10(4): 438-442.
-
Youssef AS, Capucchio MT, Rofina JE, Chambers JK, Uchida K, et al. (2016) Pathology of the aging brain in domestic and Laboratory animals, and animal models of human neurodegenerative diseases. Vet Pathol 53(2): 327-348.
-
McKenzie BA, Chen FL, Gruen ME, Olby N (2022) Canine Geriatric Syndrome: a framework for advancing research in Veterinary Geroscience. Front Vet Sci 9: 1-13.
-
Vilakartovska Z, Farbakova J, Smolek T, Hanes J, Zilka N, et al. (2021) Novel diagnostic tools for identifying impairment in dogs: behavior, biomarkers, and pathology. Front Vet Sci 7: 1-13.
-
Mondino A, Gutiérrez M, González C, Mateos D, Torterolo P, et al. (2022) Electroencephalographic signature of dogs with presumptive diagnosis of canine cognitive dysfunction. Res Vet Sci 150: 36-43.
-
Stylianaki I, Papaioannou ZS, Theodoridis A, Koutouzidou G, Baka R, et al. (2020) Amyloid-beta plasma and cerebrospinal fluid biomarkers in aged dogs with cognitive dysfunction syndrome. J Vet Intern Med 34(4): 1532-1540.
-
Landsberg Gm, Deport T, Araujo J (2011) Clinical signs and management of anxiety, sleeplessness, and cognitive dysfunction in the senior pet. Vet Clin North Am Small Anim Pract 41(3): 565-590.
-
Stelow E (2018) Diagnosis behavior problems: a guide for practitioners. Vet Clin North Am Small Anim Pract 48(3): 339-350.
-
Landsberg G, Araujo JA (2005) Behavior problems in geriatric pets. Vet Clin North Am Small Anim Pract 35(3): 675-698.
-
Pan Y (2021) Nutrients, cognitive function, and brain aging: what we have learned from dogs. Med Sci (Basel) 9(4): 72.
-
Pineda S, Olivares A, Mas B, Ibanez M (2014) Cognitive dysfunction syndrome: updated behavioral and clinical evaluations as a tool to evaluate the well-being of aging dogs. Arch Med Vet 46: 1-12.
-
Zakosek Pipan M, Prpar Michevc S, Strbenc M, Kosak U, German Ilic I, et al. (2021) Treatment of canine cognitive dysfunction with novel butyrylcholinesterase inhibitor. Sci Rep 11(1): 18098.
-
Landsberg GM, Nichol J, Araujo JA (2012) Cognitive dysfunction syndrome: a disease of canine and feline brain aging. Vet Clin North Am Small Pract 42(4): 749- 768.
-
Siwak CT, Gruet P, Woehrle F, Muggenburg BA, Murphey BA, et al. (2000) Comparison of the effects of adrafinil, propentofylline, and nicergoline on behavior in aged dogs. Am J Vet Res 61(11): 1410-1414.
-
Pan Y, Landsberg G, Mougeot I, Kelly S, Xu H, et al. (2018) Efficacy of a therapeutic diet on dogs with signs of Cognitive Dysfunction Syndrome (CDS): a prospective double blinded placebo controlled clinical study. Front Nutr 5: 1-10.
-
Pan Y, Kennedy AD, Jonsson TJ, Milgram NW (2018) Cognitive enhancement in old dogs from dietary supplementation with a nutrient blend containing arginine, antioxidants, B vitamins and fish oil. Br J Nutr 119(3): 349-358.
-
Krawiec DR (1989) Urologic disorders of the geriatric dog. Clin North Am Small Anim Pract 19(1): 75-85.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework