A Brief Narrative about Scientific Evidences Involving the Feline Triaditis
The feline triaditis is a syndrome characterized by simultaneous association of cholangiohepatitis, inflammatory bowel disease and pancreatitis. Clinical signs manifest which a nonspecific way, with the initial diagnosis being made through laboratory and imaging findings; however, definitively, only the histopathological examination of organs affected is conclusive. Therapy is instituted according to the changes presented by the cats, highlighting fluid therapy and electrolyte replacement, steroidal anti-inflammatories, analgesics, antiemetics and antimicrobial drugs.
Introduction
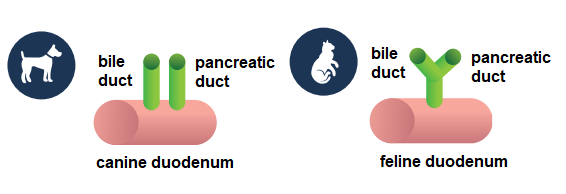
The feline triaditis corresponds to the term used to description of concomitantly presence of inflammatory bowel disease, cholangiohepatitis and pancreatitis [1, 2]. The classic concept for the development of this syndrome involves the peculiar anatomy of the feline common bile duct, which joins the main pancreatic duct before opening into the duodenum at the major duodenal papilla, favoring the rise of bacteria from the duodenum to the pancreas and liver, resulting in inflammation of the pancreas, liver, and bile duct [3].
It is believed that this anatomical arrangement also favors the transfer of antigens, toxins and microbial agents, enzymes, and proteins from the duodenum to the liver, gallbladder, and pancreas. Thus, cholangiohepatitis, inflammatory bowel disease and pancreatitis alone may favor the development of the feline triad [4].
There is no predilection for breed, sex or age, and clinical signs are nonspecific and may be intermittent in the form of anorexia, lethargy, emesis and weight loss, abnormal stools (slightly soft to watery), chronic diarrhea and jaundice [1, 2, 5]. During the physical examination of cats affected by the syndrome, abdominal palpation may suggest the presence of mesenteric lymph node enlargement, thickened intestinal walls and hepatomegaly [6].
Definitive diagnosis of feline triaditis requires histological confirmation of inflammation in each of the three affected organs. However, inflammation of more than one organ in feline clinical practice is often suspected of the feline triaditis, based on clinical, laboratory and imaging evidence [2].
Inflammatory Bowel Disease
Feline inflammatory bowel disease is a group of chronic idiopathic disorders of gastrointestinal tract, characterized histologically by the presence of leukocytes in the lamina propria inside mucosa of small intestine [6, 7]. Inflammatory bowel disease is classified second the type of leukocyte infiltrate into lymphocytic-plasmacytic enteritis, lymphocytic enteritis, and lymphocytic-plasmacytic colitis. Others fewer common forms are eosinophilic colitis or gastroenteritis, neutrophilic (suppurative) colitis, and histiocytic colitis [8, 9, 10, 11].
Different risk factors are related to the development of inflammatory bowel disease in cats, like genetic susceptibility, environmental factors, and dietary factors [12, 13, 14, 15, 16, 17]. Most felines that present with inflammatory bowel disease are middle-aged to elderly animals, and no racial or sex-linked predisposition has been described [1].
Symptoms of inflammatory bowel disease include emesis, weight loss, diarrhea, lethargy, variable appetite, and hematochezia. The presence of mucus in the stool and increased frequency of defecation are observed less frequently [5].
The differential diagnosis includes the search for nematodes, Giardia lamblia, Cryptosporidium spp., dilofilariasis, intestinal lymphoma, hyperthyroidism, feline infectious peritonitis virus (PIF), feline viral immunodeficiency (FVI), and feline viral leukemia (FeLV) [1, 5].
Cholangiohepatitis Cholangitis Complex
The cholangitis corresponds to inflammation of the bile ducts and cholangiohepatitis to the involvement of adjacent hepatocytes, forming the cholangiohepatitis cholangitis complex. It is classified based on the predominant type of leukocytes present in the inflamed tissue, hyperplasia degree and ductal fibrosis in neutrophilic cholangiohepatitis (exudative, suppurative, or acute cholangiohepatitis), and lymphocytic cholangiohepatitis (non-suppurative cholangitis, chronic cholangiohepatitis or lymphocytic portal hepatitis) [18].
The gastrointestinal disease research and standardization group of the World Small Animal Veterinary Association (WSAVA) created a classification system based on histological aspects, standardizing the terminologies used in the evaluation of liver diseases in small animals. From the new classification, the term “cholangiohepatitis” was replaced by the term cholangitis, and inflammation of the bile ducts (cholangitis) began to be classified according to the leukocyte infiltrate and histopathological findings. The categories were defined in neutrophilic cholangitis (suppurative), lymphocytic cholangitis, chronic cholangitis associated with liver parasite infection and sclerosing cholangitis [19].
The neutrophilic cholangitis is the most common form, being observed in young and middle-aged cats, with the presence of neutrophils in epithelium of bile ducts secondary to infection by bacteria ascending from the small intestine, such as Escherichia coli, Streptococcus spp., Clostridium spp. and Salmonella spp. [20, 21]. Affected cats exhibit anorexia, fever, lethargy, prostration, emesis, and diarrhea. Jaundice, hepatomegaly and abdominal pain during palpation are uncommon [5].
The lymphocytic cholangitis affects cats with median age of nine years and develops from persistent bacterial infections and liver parasite infection, with a leukocyte infiltrate composed of neutrophils and macrophages around the bile ducts. In the portal space, epithelial duct and periportal hepatic parenchyma, is observed the presence of lymphocytes and plasma cells, dilatation and thickening of the wall of the bile ducts [22, 23].
The cats affected may present emesis, jaundice, and eventually fever. Appetite is often maintained, and in some cases polyphagia occurs. About one third of cats may have ascites due to the accumulation of protein exudate, it is important to differentiate lymphocytic cholangitis from feline infectious peritonitis [18].
The cholangitis associated with liver parasites is described in felines living in endemic areas with the occurrence of trematodes of the Dicrocoeliidae family (Platynosomum spp.) [24] and Opisthorchiidae family (Opisthorchis felineus, Clonorchis spp., Metorchis albidus, Amphimerus pseudofelineus) [25, 26, 27, 28]. The trematode Platynosomum fastosum is common in subtropical and tropical regions, affecting domestic and wild felines by lodging in the bile ducts, pancreas, and gallbladder. In massive infestations, cats present jaundice, diarrhea, emesis, dehydration, ascites, extrahepatic biliary obstruction, hepatomegaly, and liver cirrhosis in terminal cases [29].
In cholangitis, laboratory findings include a decrease in serum albumin concentration, increase in the number of neutrophils in peripheral blood and increased feline pancreatic lipase serum immunoreactivity (fPLI). Increased partial thromboplastin time and serum levels of alanine aminotransferase may also occur (ALT) [5]. In some cats with cholangitis and hepatic steatosis, there is an increase in serum levels of total lipase, alkaline phosphatase (ALP), aspartate transaminase (AST), c-glutamyl transferase (cGT) and total bilirubin (TBIL) [5].
Pancreatitis
The pancreatitis corresponds to the inflammation of exocrine pancreatic tissue, classified in acute and chronic [30, 31]. The acute pancreatitis is characterized by the presence of neutrophils, interstitial edema, and peripancreatic (mesenteric) fat necrosis. In chronic pancreatitis, a leukocyte mononuclear inflammatory infiltrate and permanent microscopical structural changes such as fibrosis and pancreatic acinar atrophy are observed [32].
The hypercalcemic disorders, organophosphates intoxication, ischemia, trauma, use of glucocorticoids, infections by pancreatic parasites, feline herpesvirus, feline calicivirus, feline infectious peritonitis virus, Toxoplasma gondii, cholangiohepatitis and pre-existing inflammatory bowel disease are causes of pancreatitis [4].
The clinical presentation of cats with pancreatitis is vague and nonspecific, with presence of signals such as ataxia, lethargy, anorexia, dyspnea, dehydration, hypothermia, emesis, abdominal pain, diarrhea, and presence of palpable abdominal mass [5].
The diagnosis of feline pancreatitis is based on the clinical history and laboratory evaluation that includes blood count, serum biochemical profile, urinalysis, abdominal radiography and/or abdominal ultrasound, and specific tests of pancreatic function [33]. The laboratory alterations observed are normochromic normocytic regenerative anemia, leukocytosis, hyperglycemia, hypocalcemia, hypokalemia, hypoalbuminemia, hyperbilirubinemia, hypercholesterolemia, increased serum levels of ASP, ALT, and azotemia. The serum amylase and lipase activities are not useful in the diagnosis of feline pancreatitis, because increased values of amylase and lipase are also observed in renal and hepatic disorders, neoplasms, stress, and corticosteroid use [5, 33, 34, 35].
Etiopathogenesis of Feline Triaditis
Although the classic hypothesis involves the peculiar anatomy of the feline common bile duct, different from the canine, which empties separately into the duodenum (Figure 1) [3], it is believed that the combination of pancreatitis, inflammatory bowel disease and cholangiohepatitis presents an immune component associated with genetic (unknown at the moment) and environmental factors (bacterial infection) [1, 2, 4].
This hypothesis was initially based on cultures of bacteria Escherichia coli, Enterococcus spp., Bacteroides spp., Streptococcus spp., Clostridium spp. and Salmonella spp. from liver tissue and bile samples from cats with cholangitis/ cholangiohepatitis [36, 37], and the identification of bacteria by fluorescence in situ hybridization (FISH) in formalin-fixed tissue sections from cats with inflammatory bowel disease and pancreatitis [38].
Changes in the integrity of the intestinal mucosa support the access of bacteria, which present molecular patterns associated with pathogens (PAMPs) that interact with pattern recognition receptors (PRRs) present in the cells of the innate immune system that colonize the mucosa of gastrointestinal tract [2].
The persistence of these PAMPs [39, 40] the exposure of cryptic epitopes [41] and the molecular mimicry of bacterial antigens with host tissues [40] stimulate the synthesis of pro- inflammatory cytokines, chemokines, endothelial adhesion molecules and costimulatory molecules on the surface of antigen-presenting cells (dendritic cells, macrophages) [2].
In the intestinal mucosa, the epithelial layers, lamina propria and Peyer’s patch are rich in dendritic cells, T lymphocytes and B lymphocytes, which recognize and respond to antigens and migrate to the mesenteric lymph nodes that drain the intestine. Migration of T lymphocytes from the intestine to the liver and pancreas is facilitated by the expression of mucosal addressin cell adhesion molecule-1 (MAdCAM-1) and chemokine (C-C motif) ligand 25 (CCL25) in the intestine and liver [42, 43, 44]. Finally, local stimulation of the adaptive immune system leads to activation of self- reactive T lymphocytes and production of autoantibodies, and subsequent damage to the intestine, pancreas, liver, and biliary tract [1, 2]. The PAMPs can come from commensal bacteria or due to dysbiosis [1, 45, 46] inducing the production of IgG autoantibodies through the activation of Toll-like receptors (TLR) and receptors like nucleotide-binding oligomerization domains (NOD) receptor-like (NLR) [47].
The IgG autoantibodies against host tissue antigens (carbonic anhydrase II and lactoferrin) can be detected in autoimmune pancreatitis and chronic inflammatory bowel diseases in humans [48, 49, 50], but so far, they have not been described in felines. The nephritis in cats with cholangitis/ pancreatitis or feline triaditis is considered an age-related comorbidity [20, 51], but in humans it is considered a complication associated with inflammatory bowel disease [52] and IgG4-related disease (IgG4-RD) [53].
Diagnosis of Feline Triaditis
The concomitant diagnosis of pancreatitis, cholangiohepatitis and inflammatory bowel disease is a challenge for most veterinarians, because the three conditions cause similar clinical signs, and may occur simultaneously or separately [1, 2, 5]. During clinical examination, felines may present with fever, dehydration, hypotension, lethargy, alteration of appetite, jaundice, diarrhea, sensibility to abdominal palpation, thickening of intestinal loops and palpable liver margins [1, 2, 5].
The laboratory tests for cats with suspected feline triaditis include parasitological examination of feces, complete blood count and serum biochemical profile with albumin dosage (ALB), urea nitrogen (BUN), creatinine (Crea), alkaline phosphatase (ALP), alanine aminotransferase (ALT), c-glutamyl transferase (cGT), aspartate transaminase (AST), total bilirubin (TBIL), lipase (LIPA), calcium (Ca), phosphor (P), potassium (K) and sodium (Na) [2, 5].
Other exams include blood coagulation profile with prothrombin time (PT) and partial thromboplastin time (PTT), total concentration of thyroxine (T4), free thyroxine concentration (fT4), feline pancreatic lipase serum immunoreactivity (fPLI measured by Spec fPL), trypsin-like immunoreactivity (fTLIg), and serology/molecular biology testing for FIV, FeLV, and feline coronavirus [5].
Alterations in laboratory tests are not very specific, but regenerative or non-regenerative anemia, leukopenia, lymphopenia, thrombocytosis, increased serum levels of liver enzymes [alanine aminotransferase (ALT), alkaline phosphatase (ALP) and c -glutamyl transferase (cGT)], hypocholesterolemia, hyperbilirubinemia, hypoglycemia or hyperglycemia, hypoalbuminemia and hypergammaglobulinemia can be found [5].
Abdominal radiography does not demonstrate relevant changes in pancreatitis, liver, and kidney diseases. Radiographic examination is indicated in cases of suspected extra-alimentary disorder such as partial chronic obstruction or presence of intra-abdominal mass [2].
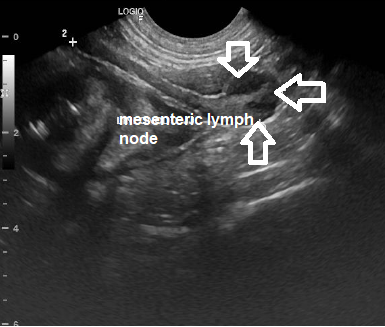
Although the literature describes a low sensitivity of abdominal ultrasound in the diagnosis of feline pancreatitis, this is a consequence of the inability of the professional who performs the examination and the quality of the equipment [1, 5]. In my clinical experience, ultrasound of the abdomen has proven to be extremely useful and fundamental in the search for alterations involving the alimentary tract that help in the diagnosis of feline triaditis. In this exam, changes can be observed, such as an enlarged and hypoechogenic pancreas (Figure 2); hepatomegaly and increased liver echogenicity (Figure 3); dysmotility and thickening of the small bowel wall (Figure 4); structural changes in gallbladder (Figure 5); and changes in the size of mesenteric lymph nodes (Figure 6).
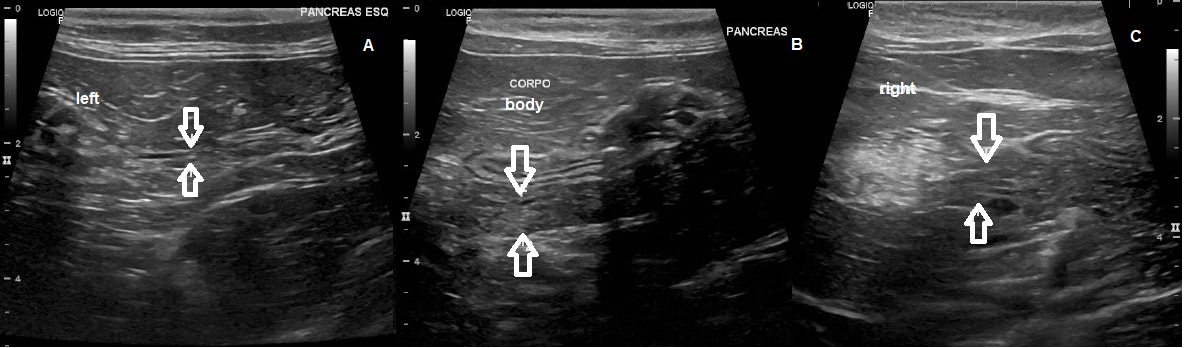
Figure 2: Ultrasound of the pancreas. A. Pancreas with normal dimensions in the left lobe measuring 0,45 cm (arrows). B. Increased dimensions in pancreatic body region measuring 0,77 cm (arrows). C. Dimensions on the right lobe measuring up to 0.94 cm (arrows), diffusely coarse echotexture, presence of oval, hypoechogenic, homogeneous images with slightly reduced echogenicity (pancreatopathy/fatty infiltrate with areas of nodular hyperplasia).
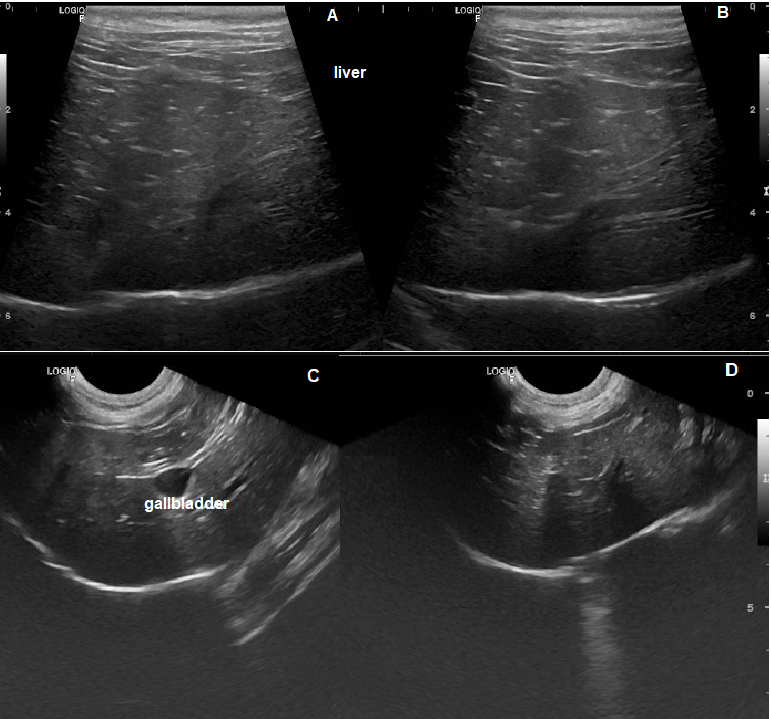
Figure 3: Ultrasound of the liver. A. and B. Liver with slightly enlarged dimensions, regular margins, slightly increased echogenicity, and preserved echotexture (hepatopathy/fatty infiltrate). C. Visualization of gallbladder. D. Liver with increased dimensions, regular margins, slightly rounded edges, maintained echogenicity and finely granular echotexture (hepatopathy).
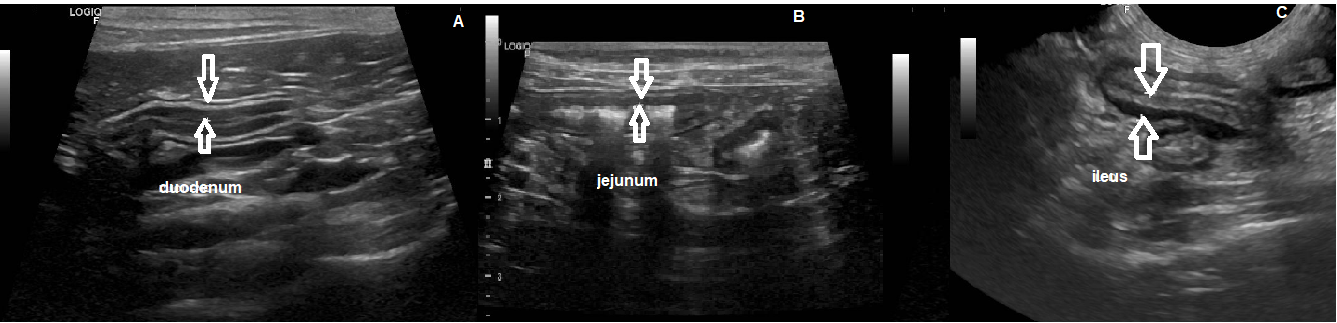
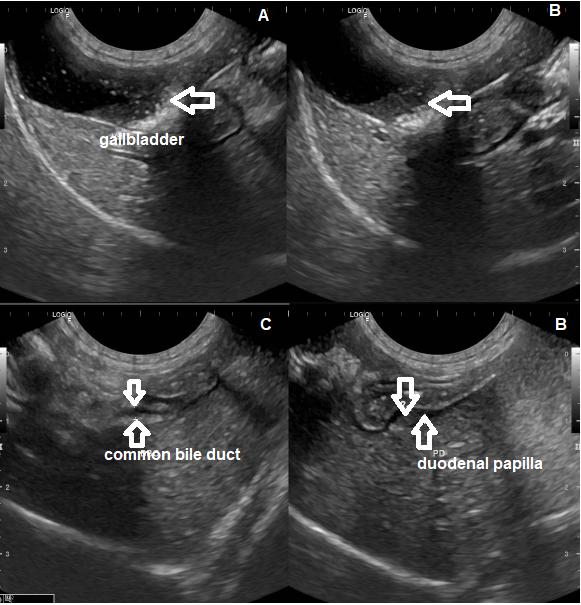
Figure 5: Ultrasound of the gallbladder. A. and B. Gallbladder with thin and regular walls, filled with anechogenic content and a discreet amount of biliary sludge with agglomerated mineral sediment/crystals interspersed, reaching up to the cystic duct (0.40 cm of diameter, arrow). C. Common bile duct without signs of dilation (0.21 cm of diameter, arrows). D. Evident duodenal papilla (0.30 cm, arrows), related with inflammatory process.
However, definitive diagnosis of the feline triad requires biopsy of all three organs by laparoscopy or exploratory laparotomy [2, 5]. Despite being invasive, laparotomy allows direct visual inspection of the organs and detection of macroscopic lesions, in addition to facilitating hemorrhage control during liver biopsy, and full-thickness tissue collection from all bowel segments, which facilitates the differentiation of intestinal lymphoma [1]. Although, this is impractical in the feline veterinary clinic due to the clinical status of the animals at the time of treatment and anesthetic risks, in addition to the non-authorization through the most tutors.
Treatment of Feline Triaditis
Each cat should be carefully evaluated, and feline triaditis treatment should be performed based on the severity of the disease present in each animal. Cats with mild symptoms can be treated at home, but those who show severe clinical signs require hospitalization and more aggressive therapy with the use of fluid therapy, antiemetics, analgesics and assisted feeding [1, 5].
The fluid therapy is one of the main key points in the treatment for feline rehydration; aims to maintain pancreatic perfusion, restore acid-base balance and colloid osmotic pressure. The calculation of total infusion volume must be based on the percentage of dehydration assessed by the responsible veterinarian, daily maintenance volume of animal and volume to correct the losses that cat presents [1].
For the control of emesis and nausea, the most used antiemetics are maropitant citrate, which acts on neurokinin (NK-1) receptors in the vomiting center and helps in visceral analgesia [54] and the ondansetron, acting on serotonin receptors (5-HT3) [55].
The analgesics are important in the treatment of the feline triaditis, because pain and nausea are largely responsible for anorexia in cats. [56]. The use of opioids such as buprenorphine [57], methadone [58] or fentanyl [59] are indicated when cats have moderate to severe pain [1, 2].
Steroid anti-inflammatory drugs such as prednisolone are indicated in the treatment of inflammatory response in the gastrointestinal system [23, 60]. The antibiotics indicated for the control and prevention of infections are the association amoxicillin+clavulanic acid, clindamycin and cephalexin associated with metronidazole. The duration of antibiotic use should be at least 3-4 weeks but can vary by up to 1-3 months [32, 61, 62]. Antioxidant and hepatoprotective medications indicated in the case of cholangiohepatitis and pancreatitis are acetyl cysteine, S-adenosyl methionine (SAMe) and ursodeoxycholic acid (Ursacol) to reduce the hepatic and biliary inflammatory response [1, 2, 23, 62].
The hypokalemia should be corrected when serum potassium levels are below 3.5mEq/L. This occurs during gastrointestinal losses due to vomiting and diarrhea. In most cases of hypokalemia, cats are asymptomatic, but some have anorexia and muscle weakness with neck ventroflexion. The hypokalemia can also lead to changes in the electrocardiogram, such as an increase in the QT interval, predisposing to premature heartbeats and arrhythmias [1, 2, 4, 63].
The vitamin B complex should be supplemented in cats with hypocobalaminaemia. The cyanocobalamin replacement is important in the treatment of feline triaditis because diseases of exocrine pancreas, liver and gastrointestinal diseases lead to sub-levels serum of cobalamin [1, 2, 64]. The use of appetite stimulants is indicated to help caloric intake, for example using mirtazapine. However, its dose in cases of significant liver disease should be reduced and its interval use should be every 48 to 72 hours [2, 55].
The enteral feeding is of great importance in the treatment of the feline triad, because prevents or corrects malnutrition and prevents the development of hepatic steatosis [1, 2, 4, 65]. It is important to be aware of the amount of food provided to prevent the refeeding syndrome, that occurs when the sudden reintroduction of food is made in animals with anorexia or malnourished, triggering severe electrolyte disturbances [66]. The enteral feeding of cats with anorexia that do not respond well to appetite stimulants and antiemetics can be performed through feeding tubes using nasoesophageal tube or esophagostomy tube [1].
The nasoesophageal tube has some advantages such as easy placement, good acceptance by most patients, who have normal ability to eat and drink, however, it has some disadvantages such as inadvertent placement in the trachea, smaller tube size and can be easily removed by the cat [66, 67]. The placement of esophagostomy tube is a simple and practical procedure in clinical veterinary routine, despite requiring general anesthesia of the patient for placement, where the tutor can continue the nutritional treatment inside home [67, 68, 69].
Conclusion
The feline triaditis is a syndrome where pancreatitis, cholangitis and inflammatory bowel disease occur concomitantly in cats. This syndrome can occur because of an infectious or autoimmune process, whose feline gastrointestinal tract anatomy promotes a greater risk of ascending bacterial infections of the liver and pancreas. The cats show nonspecific clinical signs, and the definitive diagnosis involves the histopathology evaluation of each organ, prevailing in many cases such as diagnostic suspicion. Treatment is individualized, depending on the severity of disease in each affected organ.
References
-
Cerna P, Kilpatrick S, Gunn-Moore DA (2020) Feline comorbidities: What do we really know about feline triaditis?. J Feline Med Surg 22(11): 1047-1067.
-
Lidbury JÁ, Mooyottus S, Jergens AE (2020) Triaditis: Truth and consequences. Vet Clin North Am Small Anim Pract 50(5): 1135-1156.
-
Costa PRS (2014) Tríade Felina. Revista CFMV 62: 39-40.
-
Simpson KW (2015) Pancreatitis and triaditis in cats: causes and treatment. Journal of Small Animal Practice 56(1): 40-49.
-
Fragkou FC, Adama-Moraitou KK, Poutahidis T, Prassinos NN, Kritsepi-Konstantinou M, et al. (2016) Prevalence and clinicopathological features of triaditis in a prospective case series of symptomatic and asymptomatic cats. J Vet Intern Med 30(4): 1031-1045.
-
Marsilo S (2021) Feline chronic enteropathy. Journal of Small Animal Practise 62(6): 409-419.
-
Balseiro A, Perez V, Juste RA (2019) Chronic regional intestinal inflammatory disease: A trans-species slow infection?. Comp Immunol Microbiol Infect Dis 62: 88- 100.
-
Jerges AE, Moore FM, Haynes JS, Miles KG (1992) Idiopathic inflammatory bowel disease in dogs and cats: 84 cases (1987-1990). J Am Vet Med Assoc 201(10): 1603-1608.
-
Yamasaki K, Suematsu H, Takahashi T (1996) Comparison of gastric and duodenal lesions in dogs and cats with and without lymphocytic-plasmocytic enteritis. J Am Vet Med Assoc 209(1): 95-97.
-
Day MJ, Bilzer T, Mansell J, Willcock B, Hall EJ, et al. (2008) Histopathological standards for the diagnosis of gastrointestinal inflammation in endoscopic biopsy samples from the dog and cat: a report from the World Small Animal Veterinary Association Gastrointestinal Standardization Group. J Comp Pathol 138(1): S1-S43.
-
Van Kruiningen HJ, Ryan MJ, Shindel NM (1983) The classification of feline colitis. J Comp Pathol 93(2): 275- 294.
-
Johnston KL, Swift NC, Forster-van Hijfte M, Rutgers HC, Lamport A, et al. (2001) Comparison of the bacterial flora of the duodenum in healthy cats and cats with signs of gastrointestinal tract disease. J Am Vet Med Assoc 218(1): 48-51.
-
Guilford WG, Jones BR, Markwell PJ, Arthur DG, Collett MG, et al. (2001) Food sensitivity in cats with chronic idiopathic gastrointestinal problems. J Vet Intern Med 15(1): 7-13.
-
Waly NE, Stokes CR, Gruffydd-Jones TJ, Day MJ (2004) Immune cell populations in the duodenal mucosa of cats with inflammatory bowel disease. J Vet Intern Med 18(6): 816-825.
-
Allenspach K (2011) Clinical immunology and immunopathology of the canine and feline intestine. Vet Clin North Am Small Anim Pract 41(2): 345-360.
-
Gaschen FP, Merchant SR (2011) Adverse food reactions in dogs and cats. Vet Clin North Am Small Pract 41(2): 361-379.
-
Waly NE, Peters IR, Day MJ, Stokes CR, Bailey M, et al. (2014) Measurement of IL-12 IL-23, and IFN-g mRNA in duodenal biopsies of cats with inflammatory enteropathy. J Vet Intern Med 28(1): 42-47.
-
Boland L, Beatty J (2017) Feline cholangitis. Vet Clin North Am Small Anim Pract 47(3): 703-724.
-
Cullen JM (2009) Summary of the World Small Animal Veterinary Association Standardization Committee guide to Classification of liver disease in dogs and cats. Vet Clin North Am Small Anim Pract 39(3): 395-418.
-
Callahan Clark JE, Haddad JL, Brown DC, Morgan MJ, Van Winkle TJ, et al. (2011) Feline cholangitis: a necropsy study of 44 cats (1886-2008). J Feline Med Surg 13(8): 570-576.
-
Otte CM, Penning LC, Rothuizen J, Favier RP (2011) Cholangitis in cats: symptoms, cause, diagnosis, treatment, and prognosis. Tijdschr Diergeneeskd 136(5): 332-338.
-
Warren A, Center S, McDonough S, Chiotti R, Goldstein R, et al. (2011) Histological features, immunophenotyping, clonality, and eubacterial fluorescence in situ hybridization in cats with lymphocytic cholangitis/ cholangiohepatitis. Vet Pathol 48(3): 627-641.
-
Otte CM, Rothuizen J, Favier RP, Penning LC, Vreman S (2014) A morphological and immunohistochemical study of the effects of prednisolone or ursodeoxycholic acid on liver histology in feline lymphocytic cholangitis. J Feline Med Surg 16(10): 796-804.
-
Nguyen HM, Van Hoang H, Ho LT (2017) Platynosomum fastosum (Trematoda: Dicrocoeliidae) from cats in Vietnam: Morphological redescription and molecular phylogenetics. Korean J Parasitol 55(11) 39-45.
-
Fedorova OS, Fedotova MM, Sokolova TS, Golovach EA, Koshirina YV, et al. (2018) Opisthorchis felineus infection prevalence in Western Siberia: A review of Russian literature. Acta Trop 178: 196-204.
-
Sohn WM, Chai JY (2005) Infection status with helminths in feral cats purchased from a market in Busan, Republic of Korea. Korean J Parasitol 43(3): 93-100.
-
Zhan X, Li C, Wu H, Sun E, Zhu Y (2017) Investigation on the endemic characteristics of Metorchis orientalisin Huainan area, China. Nutr Hosp 34(3): 675-679.
-
Todd KS, Bereland ME, Hickman GR (1975) Amphimerus pseudofelineus infection in a cat. J Am Vet Med Assoc 166(5): 458-459.
-
Lima RL, Pacheco RC, Mendonça AJ, Néspoli PEB, Morita LHM, et al. (2021) Platynosomum fastosum in domestic cats in Cuiabá, Midwest region of Brazil. Vet Parasitol Reg Stud Reports 24: 100582.
-
Ferreri JÁ, Hardam E, Kimmel SE, Saunders HM, Van Winkle TJ, et al. (2003) Clinical differentiation of acute necrotizing from chronic non suppurative pancreatitis in cats: 63 cases (1996-2001). J Am Vet Med Assoc 223(4): 469-474.
-
Watson P (2015) Pancreatitis in dogs and cats; definitions and pathophysiology. J Small Anim Pract 56(1): 3-12.
-
Forman MA, Steiner JM, Armstrong PJ, Camus MS, Gaschen L, et al. (2021) ACVIM consensus statement on pancreatitis in cats. J Vet Intern Med 35(2): 703-723.
-
Armstrong PJ, Williams DA (2012) Pancreatitis in cats. Top Companion Anim Med 27(3): 140-147.
-
Xenoulis PG (2015) Diagnosis of pancreatitis in dogs and cats. J Small Anim Pract 56(1): 13-26.
-
Nivy R, Kaplanov A, Kuzi S, Mazaki-Tovi M, Yas E, et al. (2018) A retrospective study of 157 hospitalized cats with pancreatitis in a tertiary care center: Clinical imaging and laboratorial findings, potential prognostic markers and outcome. J Vet Intern Med 32(6): 1874- 1885.
-
Brain PH, Barrs VR, Martin P, Baral R, White JD, Beatty JA (2006) Feline cholecystitis and acute neutrophilic cholangitis: clinical findings, bacterial isolates, and response to treatment in six cases. J Feline Med Surg 8(2): 91-103.
-
Wagner KA, Hartmman FA, Trepanier LA (2007) Bacterial culture results from liver, gallbladder, or bile in 248 dogs and cats evaluated for hepatobiliary disease: 1988-2003. J Vet Intern Med 21(3): 417-424.
-
Twedt DC, Cullen J, McCord K, Janeczko S, Dudak J, et al. (2014) Evaluation of fluorescence in situ hybridization for the detection of bacteria in feline inflammatory liver disease. J Feline Med Surg 16(2): 109-117.
-
Haruda I, Yanagisawa N, Kawamura S, Furukawa T, Shimizu K, et al. (2010) A mouse model of autoimmune pancreatitis with salivary gland involvement triggered by innate immunity via persistent exposure to avirulent bacteria. Lab Invest 90(12): 1757-1769.
-
Rojas M, Restrepo-Jimenez P, Monsalve DM, Pacheco Y, Acosta-Ampudia Y, et al. (2018) Molecular mimicry and autoimmunity. J Autoimmun 95: 100-123.
-
Warnock MG, Goodacre JÁ (1997) Cryptic T-cell epitopes and their role in the pathogenesis of autoimmune diseases. Br J Rheumatol 36(11): 1144-1150.
-
Calabrese GC, Luczak EM, Roux ME (2008) Importance of CCL25 in the attraction of T cells and the role of IL-7 on the signaling pathways in intestinal epithelial cells. Immunobiology 214(6): 403-409.
-
Schippers A, Hubel J, Heymann F, Clashsen T, Eswaran S, et al. (2021) MAdCAM-1/α4β7 integrin-mediated lymphocyte/endothelium interactions exacerbate acute immune-mediated hepatitis in mice. Cell Mol Gastroenterol Hepatol 11(4): 1227-1250.e1.
-
Wu X, Sun M, Yang Z, Lu C, Wang Q, et al. (2021) The roles of CCR9/CCL25 in inflammation and inflammation- associated diseases. Front Cell Dev Biol 9: 686548.
-
Yanagisawa N, Haruta I, Shimizu K, Furukawa T, Higuchi T, et al. (2014) Identification of commensal flora-associated antigen as a pathogenetic factor of autoimmune pancreatitis. Pancreatology 14(2): 100- 106.
-
Kinashi Y, Hase K (2021) Partners in leaky gut syndrome: intestinal dysbiosis and autoimmunity. Front Immunol 12: 673708.
-
Watanabe T, Yamashita K, Fujikawa S, Sakurai T, Kudo M, et al. (2012) Involvement of activation of toll-like receptors and nucleotide-binding oligomerization domain-like receptors in enhanced IgG4 responses in autoimmune pancreatitis. Arthritis Rheum 64(3): 914- 924.
-
Roozendaal C, Horst G, Pogany K, van Milligen de Wit AW, et al. (1998) Prevalence and clinical significance of anti-lactoferrin autoantibodies in inflammatory bowel diseases and primary sclerosing cholangitis. Adv Exp Med Biol 443: 313-319.
-
Taniguchi T, Okazaki k, Okamoto M, Seko S, Tanaka J, et al. (2003) High prevalence of autoantibodies against carbonic anhydrase II and lactoferrin in type 1 diabetes: concept of autoimmune exocrinopathy and endocrinopathy of the pancreas. Pancreas 27(1): 26-30.
-
Tan L, Zhang T, Peng W, Chen J, Li H, et al. (2014) Detection of anti-lactoferrin antibodies and anti-myeloperoxidase antibodies in autoimmune hepatitis a retrospective study. J Immunoassay Immunochem 35(4): 388-397.
-
Weiss DJ, Gagne JM, Armstrong PJ (1996) Relationship between inflammatory hepatic disease and inflammatory bowel disease, pancreatitis, and nephritis in cats. J Am Vet Med Assoc 209(6): 1114-1116.
-
Joyce E, Glasner P, Ranganathan S, Swiatecka-Urban A (2017) Tubulointerstitial nephritis: diagnosis, treatment, and monitoring. Pediatr Nephrol 32(4): 577- 587.
-
Umehara H, Okazaki K, Kawa S, Takahashi H, Goto H, et al. (2021) The 20202 revised comprehensive diagnostic (RCD) criteria for IgG-RD. Mod Rheumatol 31(3): 529- 533.
-
Park LS, Hoelzler MG (2021) Retrospective evaluation of maropitant and perioperative factors affecting postoperative appetite in cats. Can Vet J 62(9): 969-974.
-
Fitzpatrick RL, Wittenburg LA, Hansen EJ, Gustafson DL, Quimby JM (2016) Limited sampling pharmacokinetics of subcutaneous ondansetron in healthy geriatric cats, cats with chronic kidney disease, and cats with liver disease. J Vet Pharmacol 39(4): 350-355.
-
Reid J, Scott EM, Calvo G, Nolan AM (2017) Definitive Glasgow acute pain scale for cats: validation and intervention level. Vet Rec 180(18): 449.
-
Clark TP (2022) The history and pharmacology of buprenorphine: new advances in cats. J Vet Pharmacol Ther 45 (S1): 1-S30.
-
Robertson AS, Taylor PM (2004) Pain management in cats-past, present, and future. Part 2. Treatment of pain- clinical pharmacology. J Feline Med Surg 6(5): 321-333.
-
Davison CD, Pettifer GR, Henry JD (2004) Plasma fentanyl concentrations and analgesic effects during full or partial exposure to transdermal fentanyl patches in cats. J Am Vet Med Assoc 224(5): 700-705.
-
Okanishi H, Nagata T, Nakane S, Watari T (2019) Comparison of initial treatment with and without corticosteroids for suspected acute pancreatitis in dogs. S Small Anim Pract 60(5): 298-304.
-
Makielski K, Cullen J, O´Connor A, Jergens AE (2019) Narrative of therapies for chronic enteropathies in dogs and cats. J Vet Intern Med 33(1): 11-22.
-
Center SA, Randolph JF, Warner KL, Flanders JA, Harvey HJ (2022) Clinical features, concurrent disorders, and survival time in cats with suppurative cholangitis- cholangiohepatitis syndrome. J Am Vet Med Assoc 260(2): 212-227.
-
Kogika MM, de Morais HA (2017) A quick reference on hypokalemia. Vet Clin North Am Small Anim 47(2): 229- 234.
-
Toresson L, Steiner JM, Olmedal G, Larsen M, Suchodolski JS, et al. (2017) Oral cobalamin supplementation in cats with hypocobalaminaemia: a retrospective study. J Feline Med Surg 19(12): 1302-1306.
-
Collins S (2017) Nutritional support of cats with triaditis. Vet Nursing J 32: 158-160.
-
Taylor S, Chan DL, Villaverde C, Ryan L, Peron F, et al. (2022) 2022 ISFM Consensus Guidelines on management of the inapetente hospitalized cat. J Feline Med Surg 24(7): 614-640.
-
Klaus JÁ, Rudloff E, Kirby R (2009) Nasogastric tube feeding in cats with suspected acute pancreatitis: 55 cases (2001-2006). J Vet Emerg Crit Care (San Antonio) 19(4): 337-346.
-
Nathanson O, McGonigle K, Michel K, Stefanovski D, Clarke D (2019) Esophagostomy tube complications in dogs and cats: retrospective review of 225 cases. J Vet Intern Med 33(5): 2014-2019.
-
Brunet A, Bouzouraa T, Cadore JL, Hugonnard M (2022) Use of feeding tubes in 112 cats in an internal medicine referral service (2015-2020). J Feline Med Surg 24(10): e338-e346.
- California Red-Legged Frog and Non-Listed Amphibians Response to Non-Native Fish Removal
- Industrial Standardization of the Bio-OS: Algorithmic Codification of Resilience Engineering Guidelines and Version V8 Architecture
- Climate Variability and the Sustainability of Snail Farming in Nigeria: Past Trends, Present Challenges and Potential Outlook
- The Evaluation of the Surveillance System of Anthrax in Gilgit-Baltistan, Pakistan, 2018
- Natural Decline to Extinction of A New Zealand Rabbit Population
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework