Submandibular Gland Schwannoma - Case Report
Schwannomas are benign tumors that originate in the myelin sheath of neurons, more specifically in Schwann cells. Between 25-45% of these tumors occur in the topography of the head and neck, and may appear in various anatomical sites –oral cavity, larynx, pharynx, parapharyngeal space, and others. The main complaints are a painless, slow-growing mass and symptoms related to compression of nearby structures by the lesion. Its diagnosis is almost always given with the anatomopathological study after resection of the lesion, since fine-needle punctures usually show indeterminate results and imaging tests such as computed tomography (CT) and magnetic resonance imaging (MRI) cannot confirm this diagnosis, although they bring important information about location, size and contact with adjacent structures. Treatment, if there is no contraindication, is through surgical excision of the tumor. In this report, we present the case of a 47 year-old female patient complaining of left submandibular nodulation, whose diagnosis of schwannoma was only given after a left submaxillaryectomy, through the pathological examination.
Introduction
Schwannoma is a benign neoplasm that originates in the Schwann cells of the myelin sheath, which cover the nerves of the human body. They can arise in peripheral, central and autonomic nerve axons, with about 25-45% occuring in the head and neck. In this topography, there are reports of its appearance in the parapharyngeal and retropharyngeal spaces, in the paranasal sinuses and nasal cavity, submandibular region, oral cavity, larynx, among others [1]. They are encapsulated neoplasms with no predilection for sex and age, with na insidious and painless growth. The most common symptoms are related to the appearance of a nodulation and the compression it causes in adjacent structures.
For diagnosis, fine needle aspiration biopsy (FNAB) has low success rates and is mostly inconclusive [2]. Among the imaging exams, computed tomography (CT) and especially magnetic resonance imaging (MRI) are the best options despite not having high specificity rates, being, however, useful to assess the shape, size and location of the lesion [3]. It is not always possible to identify the nerve from which the tumor originates, which for some cases is of fundamental importance so that the patient can understand the changes that may appear after the lesion resection [4]. The treatment modality is complete resection of the tumor, with the possibility of nerve reconstruction depending on the affected nerve and with low recurrence rates [1].
In this report, we present the case of a 47 year-old female patient with a submandibular gland schwannoma.
Case Report
We present the case of a 47 year-old caucasian female who was referred from the Neurosurgery team to the Head and Neck Department due to the appearance of nodulation in the left submandibular region. In her personal history, she did not use continuous medication, denied smoking, alcohol consumption, previous surgeries and Family history of cancer in first degree relatives. She has been followed up with neurosurgery since 2019 due to meningioma, treated with radiosurgery and radiotherapy between March and May 2020.
Upon entering the department of the head and neck surgery, she complained of a painless nodulation in the left submandibular region noted 24 months ago, associated with dysphagia. On clinical examination, there were no apparent lesions on oroscopy and laryngoscopy. On palpation of the neck, presence of topical thyroid, fibroelastic consistency, no palpable nodules and absence of lymph nodes or other palpable nodules.
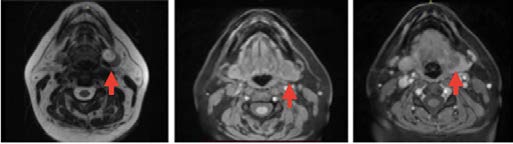
Complementary investigation with neck ultrasound was initiated, which showed a 2cm thyroid nodule in the left lobe classified as TI-RADS 4, and a regular and hypoechoic nodular formation of 3,5cm in the posterior portion of the left submandibular gland, without other worthy changes noted. Puncture of the 2 lesions was performed, the thyroid resulting from a colloid cyst and left submandibular inconclusive. This was followed by a new FNAB, again presenting an inconclusive result. A esophagogastroduodenoscopy (EGD) was also performed, which showed an elevated lesion covered by fibrina and mucus in the middle esophagus, whose biopsy showed it to be chronic ulcerative esophagitis, and a stomach polyp, which was resected and pathological compatible with a polypoid lesion. Next, neck MRI was performed, which showed a heterogeneous and well- delimited nodular lesion, which seemed to be located in the hilum of the left submandibular gland, which may correspond to schwannoma (Figure 1).
After discussing the case in a multidisciplinary meeting, it was decided to perform a left submaxillaryectomy. The patient was then submitted to general anesthesia and cervicotomy, and the left submandibular gland was identified with a nodular lesion measuring 2,5 cm. A careful dissection was performed, preserving the hypoglossal, lingual and mandibular marginal nerves. After removing the piece, a suction drain was left and the surgical wound was closed. The patient had a good postoperative evolution, being discharged on the second postoperative day.
The pathological examination confirmed with immunohistochemistry revealed a myxoid Schwannoma in a nervous sheath, with the remainder of the salivary gland without any particularities (Figure 2). Currently, the patient is under regular outpatient follow-up, with no evidence of recurrence of the lesion.
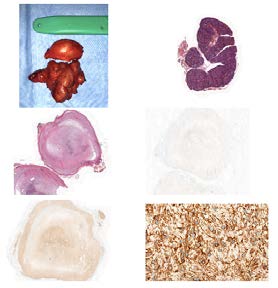
Figure 2: a) surgical speciment; b) Photomicrograph of histological section, stained with hematoxylin eosin (HE), demonstrating an image at 100x magnification of the encircled salivary gland, devoid of significant histological alterations. Image shows normal structure of serous salivary gland, containing acini distributed in lobules, with ducts showing usual distribution, between and within the lobules; c) Photomicrograph of histological section, stained with Hematoxylin Eosin (HE), demonstrating an image at 100x magnification of a nodular structure, which presents a capsule with defined limits. The structure content has a dense fibrillar component containing areas of loose pattern of this component. (Antoni A and Antoni B areas); d) Photomicrograph of histological section, used in Immunohistochemical Examination (Anti-Ki-67 Protein Antibody), demonstrating a 100x magnification image of a nodular structure, showing negativity to the exam; e) Photomicrograph of histological section, used in Immunohistochemical Examination (S-100 Anti-Protein Antibody), demonstrating a 100x magnification image of a nodular structure, showing diffuse positivity on examination; f) Photomicrograph of histological section, used in Immunohistochemical Examination (Anti Vimentin Antibody), demonstrating an image at 800 times magnification of nodular structure, showing diffuse positivity to the exam.
Discussion
Schwannomas are benign tumors that originate in the myelin sheath, more specifically in Schann cells, and can occur in any peripheral nerve in the human body. Almost 50% of these lesions occur in the topography of the head and neck, with no predilection for sex. Regarding age, the patient in our case is within the most common age of onset, between 30 and 50 years, despite the development in any time in life [4]. Given the rich nervous network present in the head and neck, there are several áreas in which this tumor can develop, including the oral cavity, larynx, pharynx, temporal and submandibular regions, parapharyngeal space, among others; coming from the cranial nerves, the most common ones affected are the glossopharyngeal (IX pair), accessory (XI) and hypoglossal (XII), while the least common is the vestibulocochlear (VIII pair) [5].
Imaging exams, mainly CT or MRI, are mandatory in the investigation of the condition, providing important information such as location, size, relationship with adjacent structures, possible identification of the compromised nerve. Magnetic resonance imaging, in particular, shows signs that are very suggestive of a schwannoma as isointense sign on T1 and increased and heterogeneous on T2 [6]. In our cause, given the depth of the lesion that was not palpated, it was the ultrasound that first showed the nodular lesion in the submandibular space, but it was the MRI that raised the greatest suspicion of the presence of a schwannoma, given the changes in signs observed in the exam, accordingly to other cases in the literature [7].
There are other case reports on submandibular gland schwannomas. Aslan G, et al [4] case report showed that the FNAB was able to give an accurate diagnosis, while in Diaz DD, et al. [8], Bansal V, et al. [9] cases, as well as in our, the FNAB was inconclusive, which meets most cases of schwannoma puncture [2, 10].
Of the available treatment modalities, the one with the best control of the lesion is surgery, since radiotherapy is insufficient to eradicate the tumor, only reducing its growth rate. As it is a neurogenic tumor, postoperative neural deficits may occur. Kang GC, et al. [5] reported that more than half of the patients who had resected head and neck Schwannomas had some degree of neurological deficit. In our postoperative follow-up, so far the patient has not presented any deficit or problem that could be attributed to tumor resection. As during the surgical procedure the hypoglossal, lingual and marginal mandibular branch of the facial nerve were identified and had no alterations, it is suspected that the patient’s schwannoma originated from an autonomic nerve that innervates the gland, which also corroborates the findings of other cases [4, 8, 9].
Conclusion
Although schwannomas are relatively common in the head and neck area, these tumors in the submandibular gland have few cases described in the literature. Bringing this diagnosis to light is intended to highlight the possibility of this differential diagnosis when faced with nodular lesions located in the submandibular space, since in the event of its occurrence, both the surgeon will be better prepared for the procedure, and the patient will be better oriented of possible postoperative complications.
References
-
Curioni OA, Souza RPD, Mercante AMDC, Jesus ACD, Pavelegeni A, et al. (2015) Extracranial neurogenic tumors of the head and neck. Braz J Otorhinolaryngol 81(6): 604-609.
-
Dey P, Mallik MK, Gupta SK, Vasishta RK (2004) Role of fine needle aspiration cytology in the diagnosis of soft tissue tumours and tumour‐like lesions. Cytopathology 15(1): 32-37.
-
Lukšić I, Müller D, Virag M, Manojlović S, Ostović KT, et al. (2011) Schwannoma of the tongue in a child. J Craniomaxillofac Surg 39(6): 441-444.
-
Aslan G, Cinar F, Cabuk, FK (2014) Schwannoma of the submandibular gland. Journal of Medical Case Reports volume 8(1): 231.
-
Kang GC, Soo KC, Lim DT (2007) Extracranial non- vestibular head and neck schwannomas: a ten-year experience. Ann Acad Med Singap 36(4): 233.
-
Beaman FD, Kransdorf MJ, Menke DM (2004) Schwannoma Radiologic-Pathologic Correlation.. Radiographics 24(5): 1477-1481.
-
Sakakibara A, Hasegawa T, Takeda D, Kusumoto J, Sakakibara S, et al. (2021) Peripheral facial nerve schwannoma at the inferior mandibular margin: J Surg Case Rep 7: 299.
-
Diaz DD, Kennedy KS, Parker GS, White VJ, et al. (1991) Schwannoma of the submandibular gland. Head & neck 13(3): 239-242.
-
Bansal V, Aggarwal P, Wadhwan V, Bansal A, Yadav M (2017) Giant Solitary Schwannoma of Submandibular Salivary Gland-A Rare Entity. J Maxillofac Oral Surg 16(3): 382-386.
-
Langner E, Del Negro A, Akashi HK, Araújo PPC, Tincani AJ, et al. (2007) Schwannomas in the head and neck: retrospective analysis of 21 patients and review of the literature. Sao Paulo Med J 125(4): 220-222.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?