A Rare Clinical Presentation of an Isolated Spheno-Choanal Polyp
Antrochoanal polyps (ACP) are more common benign polypoidal lesions arising from the maxillary sinus which grow into the maxillary sinus and extend into the choana. They occur more commonly in children and young adults; and are almost always unilateral. Polyps originating from the sphenoid sinus are rarely seen and are known as sphenochoanal polyp (SCP). Nasal obstruction and often headache are their main presenting symptoms. Computed tomography (CT), Cone beam computed tomography (CBCT), magnetic resonance imaging (MRI) and naso-endoscopic examination evaluates the presence of sphenochoanal polyp. Endoscopic removal of the spheno-choanal polyp together with the pedicle and the portion inside the sphenoid sinus is the treatment of choice. Finally, histopathology confirms the diagnosis.
Introduction
Sphenochoanal polyp is rare solitary polyp arising from the mucosa of the sphenoid sinus and for the first time it has been reported by Zuckerkandl, et al. [1, 2, 3]. It then exits through the sphenoidal ostium traverses along the sphenoethmoidal recess towards the choana reaching to nasopharynx. More than 50% of SCPs are observed in children [4]. Its main symptom is progressive nasal obstruction associated with headache and nasal discharge. They can be easily mistaken for antrochoanal polyp (ACP) and other polyp like lesions such as meningoencephalocele, nasopharyngeal angiofibroma, inverted papillomas and thornwald cyst in the nasopharynx [2, 5]. However, its main differential diagnosis is antrochoanal polyps as they are clinical and histologically indistinctive; and from its site of origin as the ACP originates from the maxillary antral mucosa [6]. Sphenochoanal polyps are of uncertain etiology but ostial obstruction of the sinus, sinus mucosal cysts, chronic inflammation and allergy are thought to be causative factors [7]. Due to its relatively deep- seated location, it often presents lately. The best way to distinguish them is with the use of Computed tomography (CT), Cone beam computed tomography (CBCT) or Magnetic resonance imaging (MRI) of the paranasal sinuses [8, 9]. Complete endoscopic removal along with its pedicle is the only treatment [10].
Clinical Presentation
A 13-year-old girl presented with the complaints of nasal obstruction, mouth breathing. Occasional breathing difficulty and mucopurulent nasal discharge for 02 years. She also complained of snoring and sleep apnea. Symptoms were gradually increasing that led to even bilateral nasal obstruction which was not improved with medication.
Anterior rhinoscopy showed a solitary, pale, greyish white shiny polypoidal mass in the anterior nasal cavity which was insensitive to touch and did not bleed on touch. The probe could pass all around it. Postnasal mirror examination revealed a huge polypoidal mass filling the whole nasopharynx.
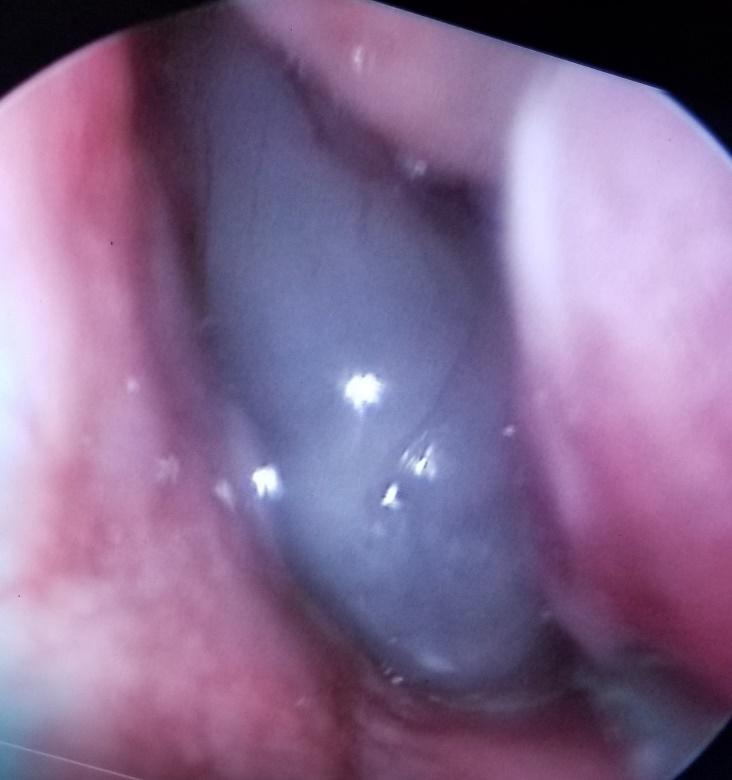
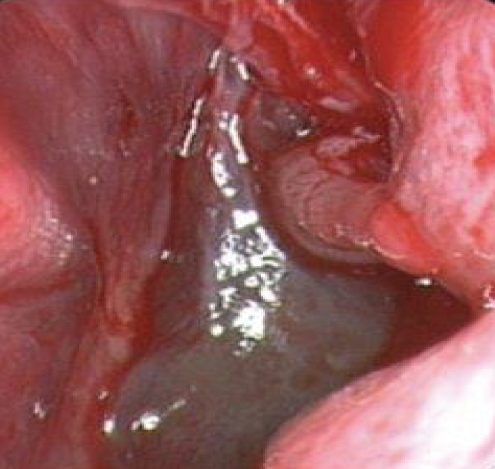
Nasoendoscopic examination revealed that a Iarge polypoidal mass in the left nasal cavity extending towards the choana occupying the entire nasopharynx causing nasal obstruction and breathing difficulty. Middle meatus was completely clear of any mass or even any secretions. However, origin of the polypoidal mass was seen coming out from the left sphenoidal ostium.
Endoscopic view.
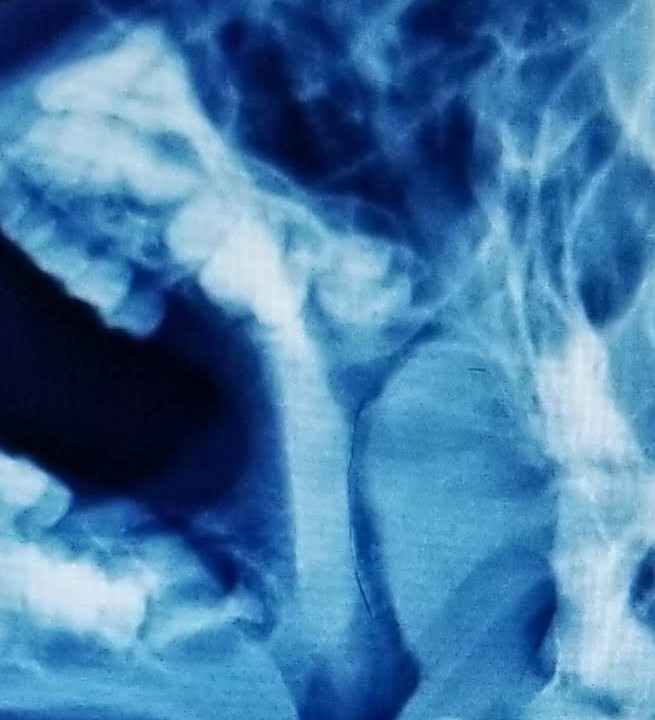
X-ray nasopharynx lateral view showed a Iarge soft tissue mass in the nasopharynx with a strip of air column behind the mass (Figure 1).
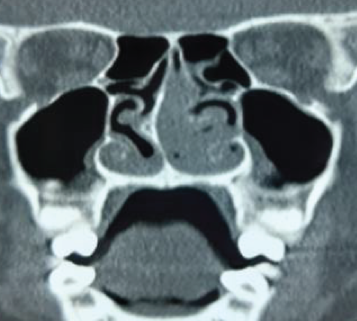
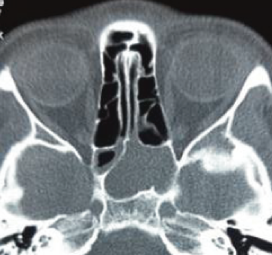
Paranasal sinus computed tomography (CT) both coronal, axial and sagittal view demonstrated a polypoid mass originating in the Ieft sphenoid sinus and extending towards the nasopharynx through the area of the spheno- ethmoid recess (Figures 2-4).
There was mild mucoperiosteal thickening in the left ethmoid sinuses, but otherwise the paranasal sinuses were clear.

Endoscopic removal of the large spheno-choanal polyp along with excision of the mucosal origin with wide opening of the sphenoidal ostium was done under general anesthesia (Figure 5) and resected mass was shown in Figures 6 & 7.


Discussion
Sphenoidal polyps are rare polyps originate from the sphenoidal sinus exit throuh the drainage ostium going through the sphenoethmoidal recess towards choana reaching to the nasopharynx [1, 2, 11]. They mainly present with nasal obstruction. It was unilateral initially but gradually obstruction became bilateral [12]. Associated symptoms are nasal discharge, snoring, mouth breathing, headache etc. In this case, she had nasal obstruction with nasal discharge, snoring and mouth breathing.
Anterior rhinoscopy is the basic step for rhinologic examination but due its deep seated location of the sphenoidal polyp, it is usually missed in anterior rhinoscopy [13]. In our case anterior rhinoscopy revealed a solitary, pale, greyish white shiny polypoidal mass in the anterior nasal cavity which was insensitive to touch and did not bleed on touch. The probe could pass all around it. There was right deviated nasal septum as the cause for nasal obstruction. Postnasal mirror examination revealed a huge polypoidal mass filling the whole nasopharynx.
Naso-endoscopic is very essential and mandatory, not only to confirm the diagnosis but also to visualize the extent of the polyp. It also evaluates the site of origin and differentiates the SCP, ACP, nasopharyngeal angiofibroma, meningoencephalocele, hemangiomatous lesion, inverted papilloma or other nasal polyposis [3, 5, 14]. In our case, O0 Karl Storz Hopkin’s rod telescope showed a Iarge polypoidal mass in the left nasal cavity extending towards the choana occupying the entire nasopharynx and the site of origin was from the left sphenoidal ostium. However, CT scan is the ‘gold standard’ examination in evaluating nasal and paranasal sinus pathology. CBCT practically is superseding CT in many cases for the diagnosis of paranasal sinus and ear diseases. MRI/MRA/ CT angiogram are done for the bony invasion, intracranial extension and vascular lesions of the nose and paranasal sinus lesions [8, 9]. The combined use of imaging techniques and diagnostic na¬sal endoscopy is suggested for accurate diagnosis of isolated sphenoid sinus lesions so that the patient can be correctly diagnosed and also get benefitted by minimally invasive techniques [12, 13].
In the presenting case initially X-ray nasopharynx lateral view was done which revealed a soft tissue lobulated mass in the nasopharynegeal region indenting the nasopharyngeal air column anteriorly with an air strip posterior to the mass. CT scan of the paranasal sinuses showed a soft tissue mass in the left spheno-ethmoidal recess extending to the choana filling the entire nasopharynx. Sphenoidal sinus was found in the left side with other paranasal sinuses particularly the left maxillary sinus. Thus, history, physical examination, paranasal imaging findings and nasal endoscopy led us to the correct diagnosis.
Functional endoscopic sinus surgery, a minimally invasive procedure is the treatment of choice for nasal and paranasal sinus polypoidal diseases that is a quite safe method of in such cases. Complete removal of the polyp both intranasal as well as intrasphenoidal component reduces the incidence of recurrence also [10, 12]. In our case endoscopic complete removal of both the components were carried out successfully. Sphenoid sinus was widened and sphenoid component was removed.
Conclusion
Nasal obstruction is the common presentation to the pediatric group of patients and antrochoanal polyp is the most common type of choanal polyp in cases of progressive unilateral nasal obstruction. Although, sphenochoanal polyp should be kept in mind in the differential diagnosis of choanal polyps. History, nasal endoscopic examination and radiology are basic to diagnosis. Endonasal endoscopic complete resection is treatment of choice.
- Acknowledgement We are grateful to Kauser Ahmed Shahin, Graphic Designer, UniMed UniHealth Pharmaceuticals Limited for his secretarial assistance.
- Conflict of interest No conflict of interest
- Funding No funding, no financial assistance
References
-
Sethi DS, Lau OP, Chee LW, Chong V (1998) Isolated sphenoethmoid reeess polyps. J Laryngol Otol 112: 660- 663.
-
Bist SS, Kumar R, Varshney S, Bisht M (2007) Isolated sphenochoanal polyp: A rare clinical entity. Indian J Otolaryngol Head Neck Surg 59(1): 56-57.
-
Mills CP (1959) Secretory cysts of the maxillary antrum and their relation to the development of antrochoanal polypi. J Laryngol Otol 73(5): 324-334.
-
Al-Qudah MA (2010) Sphenochoanal polyp: current diagnosis and management. Ear Nose Throat J 89: 311- 313.
-
Yanagisawa E, Yanagisawa K (1994) Endoscopic view of Thornwald cyst of the nasopharynx. Ear Nose Throat J 73(12): 884-885.
-
Tysome JR, Saleh HA (2007) Sphenochoanal polyp presenting with concomitant nasal polyps. Ear Nose Throat J 86(1): 50-52.
-
Ceylan A, Ileri F, Kizil Y, Uslu S, Yilmaz M, et al. (2006) Endoscopic surgery of sphenochoanal polyp. Kulak Burun Bogaz Ihtis Derg 16(2): 94-96.
-
Hayes E, Laveile W (1989) Sphenochoanal polyp: CT findings. J Comput Assist Tomogr 13(2): 365-366.
-
Weissman JL, Tabor EK, Curtin HD (1991) Sphenochoanal polyps: Evaluation with CTand MR imaging. Radiology 178(1): 145-148.
-
Maldonado M, Alobid I, Bernal-Sprekelsen M, Mullol J (2006) Sphenochoanal polyp. Diagnostic and therapeutic aspects. Acta Otorhinolaringol Esp 57(3): 149-151.
-
Ozcan M, Ozlugedik S, Ikinciogullari A (2005) Simultaneous antrochoanal and sphenochoanal polyps: a rare clinical entity. J Laryngol Otol 119(2): 152-154.
-
Lim WK, Sdralis T (2004) Regression of a sphenochoanal polyp in a child. Laryngoscope 114(5): 903-905.
-
Tosun F, Yetiser S, Akcam T, Ozkaptan Y (2001) Sphenochoanal polyp: endoscopic surgery. Int J Ped Otorhinolaryngol 58(1): 87-90.
-
Kumral TL, Yildirim G, Uyar Y (2012) Sphenochoanal polyps and the optic nerve. Clin Pract 2(1): e10.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?