Well Diving is Not Well for Hearing: Sudden Sensory Neural Hearing Loss-A Case Report
Background: Sudden sensory neural hearing loss can be caused by many factors. It may range from minimal to profound degree of hearing loss. Barotrauma is a type of ear damage caused by pressure difference between the atmosphere and the inner ear. This may result in permanent sensory neural hearing loss. Objective: The aim of the study was to use behavioral and electrophysiological assessments to analyze the hearing of a patient who experienced sudden hearing loss following a dive in well. Case Report: A 31 year old male adult who reported sudden hearing loss following a dive in the well was evaluated. Hearing assessment was done. Pure tone audiometry revealed bilateral profound hearing loss. Immittance audiometry showed ‘A’ type tympanogram in both ears and acoustic reflexes absent in both ears. In ABR click stimulus test, no responses were observed till 105dBnHL in both ears. DPOAE’s were also absent in both ears. Vestibular assessments (subjective and objective) were also done. Conclusion: The current case study verifies the importance of audiological assessment for divers and importance of safety measures to be taken.
Introduction
Barotrauma was coined to describe the compression of gases at depth and its impact. Barotrauma may affect inner ear and middle ear. If the diver descends without properly equalizing the pressures within middle ear, both the surrounding pressure and inner ear pressures increase as depth increases. The inner ear pressure increases because it is fluid filled and ambient pressure is freely transmitted to and through the fluid. When the descending diver feels discomfort rather than rising to a comfortable depth the usual response is to attempt a forceful equalization with a valsalva maneuver. When the pressure in the middle-ear space is properly equalized, the risk of inner-ear barotrauma is extremely low. If the pressure in the middle ear is not equalized during descent, the water pressure on the eardrum transfers inward through the middle-ear ossicles to the oval window, and this causes the round window to bulge outward.
The pressure itself may damage sensitive inner-ear structures. If the pressure is excessive, either the oval window or, more commonly, the round window may tear, and the inner-ear fluid (perilymph) may leak into the middle ear (perilymph fistula). Pressure waves alone can cause damage to the inner ear without window rupture.
If the rupture occurs the loss of fluid from inner ear leads to damage of the hearing organ and sometimes of the balance organ. If the leak is not stopped, it results in permanent hearing loss. The divers also experience vertigo, tinnitus, nystagmus and aural fullness.
The aim of the present study was to examine a case of barotrauma following a dive in a well.
Case Presentation
A young adult male, 31years old came with a complaint of sudden hearing loss following a dive in the well on November 2019. The patient came for ENT and audiological evaluation 3 days following the incident. The major complaints were aural fullness, giddiness, ringing sensation and one episode of vomiting since past 3 days following a incident of diving. ENT evaluation revealed bilateral tympanic membrane intact. Audiological evaluation consisted of Pure Tone Audiometry, Emittance Evaluation, Oto-Acoustic Emissions, ABR and VEMP [1, 2, 3].
Pure Tone Audiometry
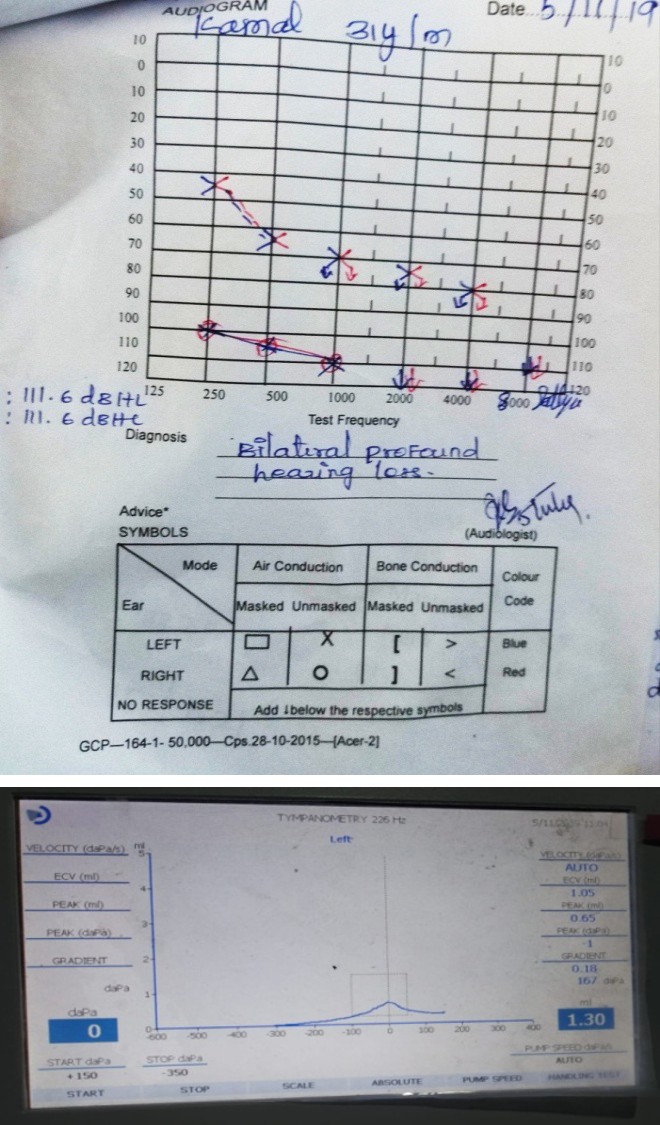
Puretone audiometry (PTA) involved air conduction thresholds from 250 to 8000Hz and bone conduction thresholds from 250 to 4000Hz. It revealed profound hearing loss in both ears. Pure tone audiometry was done in a sound treated room with Maico40 audiometer, TDH-39 headphones and B-71 bone vibrator. It revealed profound sensory-neural hearing loss in both ears [4].
Immittance Audiometer
Immittance audiometer was done using Resonance R36M instrument. Tympanometry and acoustic reflex testing were done. ‘A’ type tympanogram was obtained with reflexes absent in both ears [5].
Oto Acoustic Emissions (OAE)
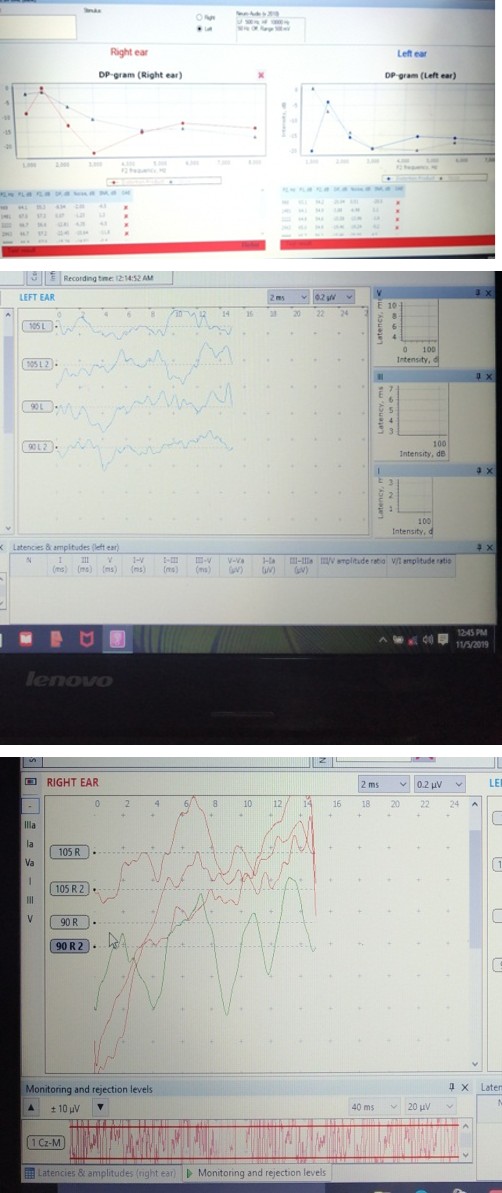
OAE was done in sound treated room with Neurosoft OAE instrument .OAE’s were absent in both ears due to higher degree of hearing loss and it indicated inadequate functioning of outer hair cells in the cochlea.
Click Auditory Brainstem Response (Click ABR)
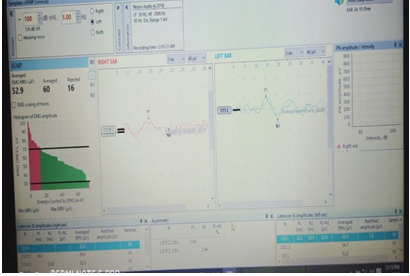
ABR was done with Neuroaudio ABR instrument. To
investigate the integrity of the auditory pathway, click ABR was performed. No replicable peaks were present in both ears at maximum intensity of 105dBnHL.
Vestibular Evoked Myogenic Potential
VEMP was done with Neuroaudio VEMP instrument. Cervical vemp and ocular vemp was performed to learn about the functioning of otolith organs, vestibular nerve, vestibulo - collic and vestibulo-ocular pathway. C-Vemp was observed to be within normal limits in both sides. The patient had ophthalmic issues like bilateral upward gazerestriction; Exopthalmos in right eye; Ptosisin left eye. He was unable to carry out the instructions given for O-VEMP and hence O-VEMP couldn’t be assessed.
Behavioral Vestibular Functional Test
Fukuda Stepping Test
It is used to identify the presence of peripheral vestibular impairment. Thepatient was instructed to march in a fixed position for 50 steps with eyes closed, arms extended outward in front of the body (palms down). The test result was recorded positive because a sway was noticed while performing the test.
Romberg Test
It is a test for static balance that assesses the function of lower spinal reflexes by facing the subject to rely on Vestibular and proprioception input to maintain upright position. The patient was asked to remove his footwear and stand with feet together and arms folded together with eyes open for 30 seconds. If the patient can perform this with eyes open, it should be repeated with eyes closed. Patient has to keep the balance for 30 seconds. If not, the result is recorded as positive. The patient was able to do the test with eyes open so the test was repeated with eyes closed. The result was positive because a sway towards right side is seen.
Discussion
Barotrauma usually causes damage to inner ear and middle ear and result in sudden sensory-neural hearing loss.
In the present study a 31 year old male who suffered sudden hearing loss and vestibular symptoms following a dive in well were analyzed.
After the client reported to hospital 3 days following the incident he was admitted in ENT ward, three courses of Intravenous injection and two courses of Intratympanic injections in both ears were given to the patient . Again a complete audiological evaluation was done to the patient. Following the course of treatment, there was improvement in his vestibular symptoms but there was no improvement in hearing.
References
-
Eggorment JJ (2017) Hearing Loss. Causes, Prevention and Treatment.
-
Kara E (2011) Sensorineural hearing loss: New insights for the health care professional.
-
Shupak A, Doweck I, Greenberg E, Gordon CR, Spitzer O (1991) Diving related inner ear injuries. Laryngoscope 101(2): 173-179.
-
Parell Joseph G (1990) Inner ear Barotrauma in Divers.
-
Clinchy A Richard (1996) Dive-The First Responder.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?